

August 4th, 2020 – Since this post was originally published I have published in this area with one of our former trainees and current fellow in Toronto M. Durst. Her paper Atypical case of preterm ovarian hyperstimulation syndrome is available through the link in full text via open access!
Thus far in my career, I have been called to the bedside to look at a female ex-preterm infant several times due to the complaint of swelling that usually extends from the lower abdomen to the upper thighs. Usually the clitoris and hood are swollen as well and at times raises the suspicion of cliteromegaly. The enlarged clitoris then prompts the question of whether the patient could be virilized from Congenital Adrenal Hyperplasia or perhaps even be male in extreme cases. As I think back on some of these babies, nursing often has expressed concerns that the infants are uncomfortable and have either been treated with furosemide (unsuccessfully) or pain medication for the perceived discomfort.
As you might expect from the first paragraph I believe I have found the answer which came to me through a circuitous route. We had a patient in the hospital recently whose phallus was small for his gestational age. After consulting the Pediatric Endocrinologist on service we performed a hormonal workup which excluded hypogonadotropic hypogonadism (small phallus due to a lack of male hormones) and insensitivity to testosterone. Our Neonatal service was advised that this child would likely experience penile growth during “Mini Puberty” I don’t know about you but I had never heard of the term so I began a search that culminated in me writing this post to hopefully bring others up to speed.
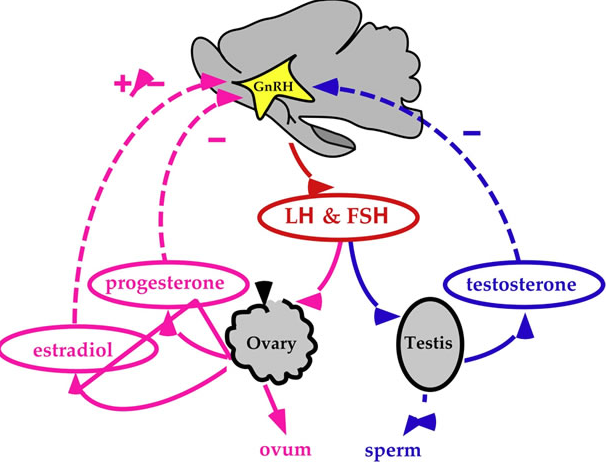
Mini puberty is secondary to the normal rise in testosterone that occurs after delivery. In utero both estrogen and testosterone inhibit GNRH with estrogen from the placenta being the most potent inhibitor. Once the placenta is removed this inhibition is lost leading to LH and FSH levels rising which peak between the 4th to 10th week that finally begin to decline after 7 months of age. The level of testosterone similarly peaks by 3 months and reaches pre-pubertal levels by 6-9 months. During this time there is an increase in testicular volume and less so penile length but a patient such as ours might reach a normal length with such stimulation if the length was not extremely short before “Mini Puberty”.
In female infants it is somewhat different in that pre-pubertal levels of estradiol are reached by two months of age. Given the lack of stimulation from excessive levels of estradiol how can we tie this back to the question of genital swelling?
In 1985 Sedin G et al published a case series of 4 premature infants who demonstrated swelling of the lower abdomen, labia and upper thighs.  In each case the etiology was found to be the same; estradiol producing ovarian cysts. In one case the cyst was removed and with it the edema resolved and in the other cases progesterone was utilized to suppress production of Gonadotropin Releasing Hormone (GNRH) and with it production of FSH and LH, thereby reducing the estradiol levels. Ultrasound in each case also revealed uterine enlargement consistent with over stimulation. What is it that causes this phenomenon is unknown for sure but it is certainly curious that the condition only seems to affect preterm infants born at < 29 weeks. Furthermore the timing of the edema is consistently at 36 – 39 weeks CGA. Sedin postulates that the reason for this is that the hypothalamic pituitary axis is immature in these preterm infants and does not provide the negative feedback to reduce LH and FSH compared to the term infant in which such sensitivity is present.
In each case the etiology was found to be the same; estradiol producing ovarian cysts. In one case the cyst was removed and with it the edema resolved and in the other cases progesterone was utilized to suppress production of Gonadotropin Releasing Hormone (GNRH) and with it production of FSH and LH, thereby reducing the estradiol levels. Ultrasound in each case also revealed uterine enlargement consistent with over stimulation. What is it that causes this phenomenon is unknown for sure but it is certainly curious that the condition only seems to affect preterm infants born at < 29 weeks. Furthermore the timing of the edema is consistently at 36 – 39 weeks CGA. Sedin postulates that the reason for this is that the hypothalamic pituitary axis is immature in these preterm infants and does not provide the negative feedback to reduce LH and FSH compared to the term infant in which such sensitivity is present.
Additionally another theory is that vascular endothelial growth factor released from ovarian granulosa and thecal cells may be involved. Since the report by Sedin, Starzyk et al have reported an additional 9 patients with such edema and ovarian cysts http://www.ncbi.nlm.nih.gov/pubmed/19039238
I suspect that many Neonatal units across the World have encountered such patients and tried a collection of treatments including furosemide or other diuretics along with fluid restriction. Unfortunately there has not been widespread description of such patients and it is my hope that with this post, awareness will increase of both “Mini Puberty” and “Genital Edema in females”. What is really needed in the latter is consultation with Endocrinology to perform provocative Hypothalamic Pituitary Axis testing and an ultrasound to confirm the presence of uterine hypertrophy and cysts. Treatment with progesterone or some other inhibitor of the GNRH will likely bring about resolution in a timely fashion without exposing the infant to a multitude of testing. Lastly such infants are often described as appearing uncomfortable which may be related to the ovarian cysts or the swelling but in either case adequate analgesia should be provided.
This truly is a post that I hope is shared with others so that we can increase awareness as there are certain to be cases in units right now that might do well to understand this condition.
Hi Michael,
Putting on my peds endo hat to clarify things for your readers regarding the normal term baby:
The Hypothalamic-Pituitary Gonadal axis is active before birth; the prenatal testosterone is necessary for baby boys to look different from baby girls. Birth actually triggers an initial drop in testosterone levels before its secretion rises again, peaking at 3 months of age as you said. Three months of age is a great time for a testosterone blood test that may obviate the need for dynamic H-P-G axis testing.
Best regards,
Shayne
Thanks!