by All Things Neonatal | Jul 30, 2015 | Neonatal, Neonatology, Pregnancy
The benefits of antenatal steroids before preterm birth have been clearly demonstrated in the literature and have been nicely summarized in a Cochrane Review. From this report the evidence is clear. Treatment with antenatal corticosteroids prior to preterm birth is associated with an overall reduction in neonatal death (relative risk (RR) 0.69, 95% confidence interval (CI) 0.58 to 0.81, 18 studies, 3956 infants), RDS (RR 0.66, 95% CI 0.59 to 0.73, 21 studies, 4038 infants), cerebroventricular haemorrhage (RR 0.54, 95% CI 0.43 to 0.69, 13 studies, 2872 infants), necrotising enterocolitis (RR 0.46, 95% CI 0.29 to 0.74, eight studies, 1675 infants), respiratory support, intensive care admissions (RR 0.80, 95% CI 0.65 to 0.99, two studies, 277 infants) and systemic infections in the first 48 hours of life (RR 0.56, 95% CI 0.38 to 0.85, five studies, 1319 infants).
While it is clear that corticosteroid administration prior to 37 weeks has great benefit, the question is whether these benefits might actually extend to 37 and 38 weeks. It has been known for some time that having an elective c-section before 39 weeks exposes the infant to an increased risk of pulmonary morbidity and NICU admission. In 2009 Tita At et al studied 24077 repeat elective c-sections at term finding that 36% were performed prior to 39 weeks. The findings conclusively demonstrated that delivery at 37 and 38 weeks increased the likelihood of a composite outcome of death or respiratory complications, treated hypoglycemia, newborn sepsis and admission to the NICU. 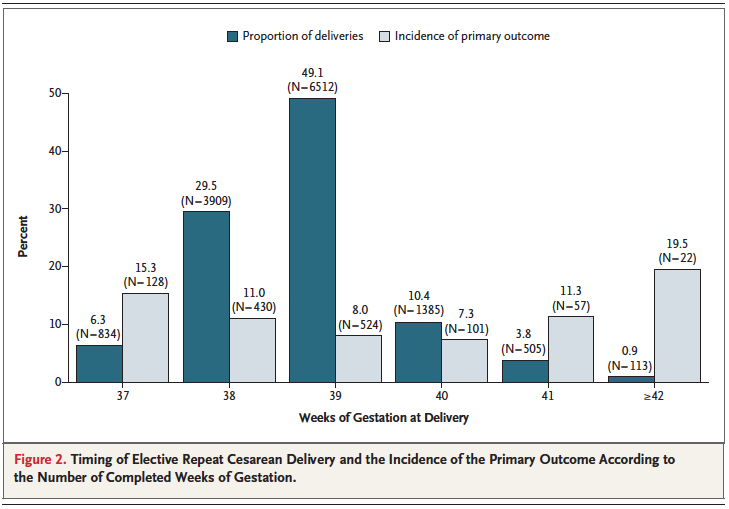 Interestingly one can also see that after 40 weeks these complications rose again. Post term deliveries are not without their consequences either.
Interestingly one can also see that after 40 weeks these complications rose again. Post term deliveries are not without their consequences either.
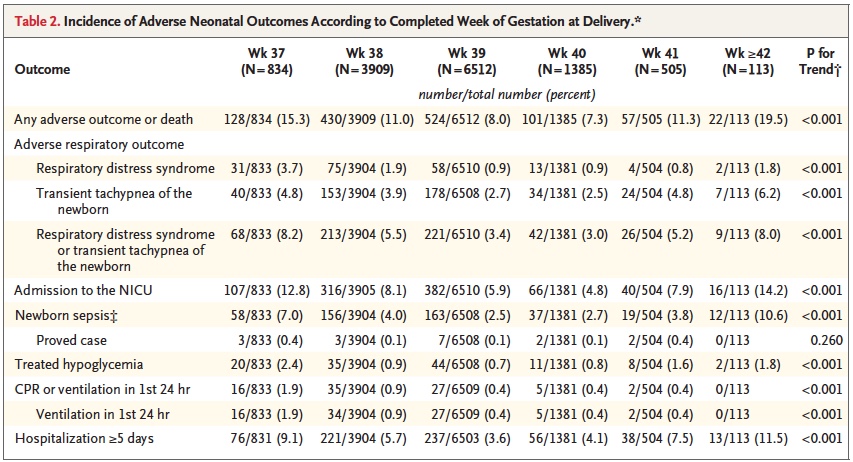
Broken down by outcome, it is also clear that each component has an increased risk at both 37 and 38 weeks compared to delivery at 39 or 40 weeks.
With such increased risk this practice has been discouraged by many obstetrical organizations including the American College of Obstetricians and Gynecologists.
Knowing that there is clear benefit to providing corticosteroids before 37 weeks, it was only a matter of time before someone would test the hypothesis that treatment of women having an elective c-section in would reduce the incidence of respiratory complications such as TTN and RDS. Surprisingly there is really only one relevant study on this subject performed by P. Stutchfield et al in 2005 entitled Antenatal Betamethasone and Incidence of Neonatal Respiratory Distress After Elective Caesarean Section: A Pragmatic Trial. The trial provided betamethasone as a single course of two doses 24 hours apart starting 48 hours before a planned c-section with 998 participants in total. 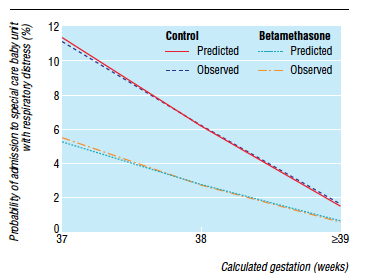
The primary outcome in this trial was admission to NICU with respiratory distress. While the study was unblinded, the results were impressive and shown in the figure to the right indicating that below 39 weeks there was a significant difference in likelihood of admission for respiratory distress if women were treated with betamethasone prior to elective delivery via c-section. In terms of effectiveness this translates to the need to treat 37 women at 37-38 weeks with betamethasone to prevent one admission for respiratory distress to NICU. Eighty percent of the newborns in the control group had TTN versus RDS so I would expect you would need to treat about 200 women to prevent one case of RDS at this gestational age. Is it worth it? I suspect if you told parents that you could prevent hospital admission of their newborn at all many would choose to do so. There is another side to this though that one must consider and that side is the impact on neurodevelopment.
Corticosteroids work by overcoming the maternal capacity to break down cortisol by a placental enzyme 11β-hydroxysteroid dehydrogenase type 2 (11β-HDS-2). Furthermore the corticosteroids used (betamethasone and dexamethasone) are resistant to degradation by this enzyme. In the brain this enzyme exists as well and has increased activity such that levels of active cortisol in the brain are at a minimum. In animal models, high levels of glucocorticoids cause decreased brain differentiation with reduced neurogenesis. These processes are likely to be similar in humans given the presence of the same enzyme which has little effect in inactivating these synthetic medications.
Even with this knowledge, we as health care providers freely recommend antenatal steroids to women at risk of preterm birth for all the benefits outlined at the start of this post. Preterm infants are at significant risk of IVH, PVL, NEC, PDA and many other conditions which in and of themselves have been linked with adverse neurodevelopment. It is the avoidance of these outcomes which likely explains why corticosteroid administration with it’s known effect on the developing brain leads to improved neurodevelopmental outcome. The challenge here is that can we extrapolate this to the 38 and 39 week fetus? I would suggest that this is not the case as the risks of the conditions leading to neurodevelopmental impairment are magnitudes less. We are then exposing these fetuses to the potential harm or glucocorticoids without the benefit of reducing the conditions that matter to outcome. On the other side of the scale is a reduction in TTN/RDS and admission to the NICU but is it worth treating 37 mothers to avoid this with the heavy weight on the other side?
If you believe I am making some unfair assumptions it is worth seeing what happened to the patients in the 2005 study by Stuchfield when they were followed up between 8 – 15 years of age. The study used a questionnaire to address a number of outcomes related to education, atopy and behaviour. The response rate for the study was only 51% of the original cohort so any conclusions must be taken with a grain of salt. That being said the authors state that there were no differences in outcome or difference in rates of asthma and atopy. In their conclusion they affirm that based on the lack of differences in long-term outcomes but with improved short-term respiratory status at birth steroids should be provided before elective c-sections. Curiously though the authors do not address an interesting finding shown in table 2 from the article.
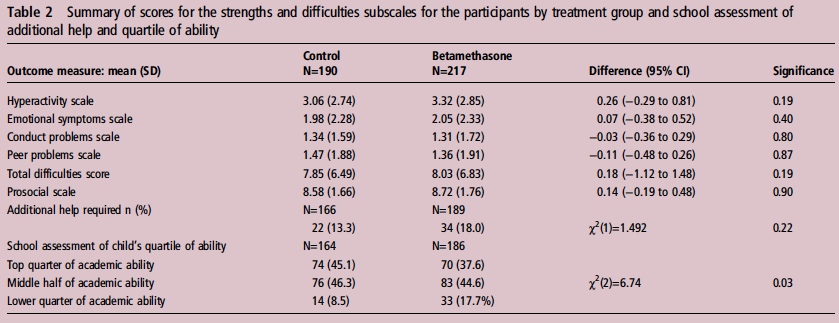
Looking at the bottom section pertaining to the school’s assessment of a child’s academic ability, less children in the steroid group performed at the top quarter of the class and twice as many children were in the lower quarter of the class. To me at least it seems disingenuous to claim no differences were seen when clearly here is a difference based on a third-party (the teacher) that is significant. The academic purists will be quick to point out that this is a secondary analysis and not the primary outcome specifically of the study and that the numbers are small. Additionally one can also argue that at a 51% response rate we are missing a great deal of outcomes. Furthermore it may well be that when it comes to surveys, those who have concerns about their participation in the study may be more apt to complete it skewing the results.
I will allow all these arguments as it really helps to support my conclusion on all of this. There is very little data out there on the benefit of providing antenatal steroids at term before elective c-section. The data out there for long-term effects does show a concern regarding school performance and the exposure in this case is to medication which is known to have effects on the developing brain. That data though is suspect as well given the issues raised in the above paragraphGiven the number of women that need to be treated to avoid one admission for respiratory distress and with the above mentioned concerns I believe more studies are needed to determine whether this is worth instituting as standard practice. Finally, any future studies will need to address in a prospective manner using a large number of patients whether there is indeed any impact on development in the long-term from such practice.

by All Things Neonatal | Jul 27, 2015 | Neonatal, Neonatology
Go to any NICU these days and you will no doubt hear about the toxicity of oxygen. Oxygen as we say is a drug and like any such product has both good and bad effects. On the good side is the ability to increase the fraction of inspired oxygen to deal with transient changes in observed saturations. In extreme cases where the patient is desaturating into the 20’s and 30’s with accompanying bradycardia this can be life saving. On the other hand the “bad” is related to toxicity from oxygen free radicals which can increase rates of ROP, BPD and in the case of resuscitation with O2 vs room air may increase the chances of death.
It is for this reason that NICU teams pay particular attention to saturation targeting. The optimal goal remains elusive as oxygen restriction to 85-89% has been linked to higher mortality as in the Support Trial (full article) while higher saturations may increase the rate of ROP and BPD. Many units are falling somewhere in the middle such as goals of 90-95% or as in our units 88-93%. If during your visit to an NICU you were to observe the nurses at the bedside you would see them or the Respiratory Therapists tweaking the oxygen up and down many times a day as they strive to keep the saturations within these ranges. As a Neonatologist I greatly appreciate the efforts of everyone on the team who try to keep maintain these goals but in the end how do they really do?
This was the subject of a 2006 paper by Hagadorn et al. Eighty four infants from 14 centres all less than 28 weeks were enrolled in this study looking at how successful staff were at keeping infants within a desired range. The findings were somewhat discouraging in that 16-64% of the time saturations were in range, while 20-73% of the time they were above range depending on the centre studied. In a different study by Laptook et al published in the same year, the results were not much better with saturations higher than goal about 15% of the time and lower by nearly 26% of the time. What impact might swings in oxygen saturation have on the brain when the saturations are low and similarly on rates of BPD and ROP when the tendency is to overshoot the goals? There is no doubt that everyone is trying to do a good job but how deflating is it to nursing and other staff members when despite their best efforts they are only in range about 60% of the time?
Fortunately I believe change is coming. With improvements in technology it is now possible to have a closed loop system in which a patient who is receiving oxygen has their saturation measured and the information via a feedback loop triggers an automated response. This response either raises or lowers the FiO2 in an automatic way which eliminates the need for health care staff to make such changes. Such technology is actually not that new as it was tested in 2001 by Claure et al and was found to be at least as effective as manual changes by a dedicated nurse. Several other small studies followed, all demonstrating an improved accuracy in maintaining target saturations. This July the same group published the following article Automated versus Manual Oxygen Control with Different Saturation Targets and Modes of Respiratory Support in Preterm Infants. This study compared the accuracy in maintaining saturations using a target of 91-95% and another of 89-93% with 80 patients participating. Patients in this study received both invasive and non-invasive ventilation. When comparing the two target ranges the automatic adjustments showed greater benefit with the results being 62 +/- 17% vs 54 +/- 16% for the 91-95% range and 62 +/- 17% vs 58 +/- 15% in the lower range. Both of these results were statistically different with p values of <0.001. When looking at episodes of significant hypoxemia as defined by a saturation < 80% the findings were interesting showing in the high range 13 vs 4 and in the low range 15 vs 4 favouring the use of autosaturations. The authors were surprised at the lack of large disparity in the accuracy between manual and auto adjustment of FiO2 but this may be related to the Hawthorne effect. Since the nurses in this study were not blinded to the intervention they may have changed their behaviour in essence to try and prove that they were just as good. How this would translate into a real world situation when a study is not being performed I suspect would favour the automated system more.
Perhaps the most interesting part of the study though was the number of Manual FiO2 adjustments per 24 hours between the two groups. For the 89%-93% SpO2 target range this was 1 [0-3] vs 102 [73-173], P < .001 and for the 91%-95% SpO2 target range 1 [0-3] vs 109 [79-156], P < .001. For me this is the crux of the discussion. In a twenty four hour period there is a reduction of about 100 interventions using the saturation range similar to our own. Take note as well that some patients required over 150 interventions in 24 hours as 100 was the mean! While the targeting is improved somewhat with the use of the auto FiO2 adjustment this is where the biggest benefit to the patient lies as I see it. Nurse and respiratory therapists are very busy on any given shift. One hundred adjustments a day translates into 4 changes in FiO2 per hour on average. Although not measured I can’t help but wonder what impact these interruptions have on the rest of the care for a given patient. What is the “ripple effect” of such interruptions in a person’s train of thought. Could this translate into a med error or delay care for another patient to whom the nurse is responsible for as well? If one didn’t have to pay as much attention to the FiO2, what other goals could their attention be put towards? Might this provide them with more time to educate parents, do skin care, or a host of other responsibilities which in the current state get interrupted every time an alarm goes off.
As this technology is improved I see this being a welcome addition to the NICU. As with anything though that promises a hands free environment it will be essential to have an override built in. Furthermore we can never take our eyes off the patient as no matter how safe these systems may be there is always the chance that a computer will freeze as we all know. The impact of such a “glitch” in the algorithm that these systems use could be catastrophic to outcome so as good as these may be we will always need the human presence to ensure that what we think we are getting from the system is actually there.

by All Things Neonatal | Jul 25, 2015 | Neonatology, resuscitation
Anyone who attends the delivery of high risk newborns will eventually encounter a baby who is born “flat”. Most of these babies will respond to stimulation and for those that don’t, the vast majority of the remaining group will come around with the use of positive pressure ventilation. The remaining infants thankfully are the rare group but these are the ones that have the highest likelihood of dying or being severely impaired and therefore leave little room for error in their resuscitation if we hope to achieve a good outcome.
In 1816 Rene Theophile Hyacinthe Laennec  invented the stethoscope to listen to the sounds of the heart and lungs. It is hard to believe that this coming year marks 200 years since that discovery and even harder to believe that when it counts most, this device still remains the best tool at your fingertips. When resuscitation has moved past the initial steps there is really nothing that can replace it’s accuracy when the going gets tough.
invented the stethoscope to listen to the sounds of the heart and lungs. It is hard to believe that this coming year marks 200 years since that discovery and even harder to believe that when it counts most, this device still remains the best tool at your fingertips. When resuscitation has moved past the initial steps there is really nothing that can replace it’s accuracy when the going gets tough.
The most recent NRP guidelines recommend that all neonates who are receiving PPV have a preductal O2 pulse oximeter placed and oxygen titrated to the amount required to keep saturations within a range based on the age of the patient. Heart rate will be displayed when such monitoring is applied as well as when chest leads are placed giving you two readings of heart rate to compare. Such comparisons often prove useful when trying to determine if the displayed saturation is an adequate result. When looking at the recommendations from the NRP there is the clear statement that the best way of determining the heart rate is through auscultating the precordial pulse but does this always happen?
The answer as you might expect is no. Quite often during resuscitation I am told what the heart rate is based on the monitor. There is a danger in relying on such technology as you will see below. Recently I was called to the resuscitation area after the delivery of a non-vigorous infant. The patient was not responding to positive pressure ventilation as determined by the colour of the patient , which was dark purple despite confirmation of tube placement by end tidal capnography. The team was guiding their continued PPV without compressions based on the monitor which was showing a heart rate of 120-130 beats per minute and the belief that they had palpated a pulse. After hearing this and recognizing that the patient before me did not fit the reading on the monitor I reached for the stethoscope. The finding of no audible heart rate prompted us to start chest compressions.
What concerned me about this case was that the presence of technology actually hindered the institution of advanced resuscitation techniques. In the last few years much of the attention in the NRP program has shifted to monitoring during resuscitation. There have been many investigating the role of O2 saturation targeting, comparisons of chest leads versus pulse oximeters for acquisition of heart rates and stressing of the importance of attaching the probe to the patient and then to the monitor to improve signal acquisition times. This patient was in Pulseless Electrical Activity (PEA) which went unrecognized due to an adequate heart rate being visualized on a monitor in the context of a non-congruent clinical exam. PEA is a state in which the heart is still experiencing electrical conduction but there is not enough contractility to eject blood.
Another interesting aspect to this case was the claim that the infant had an adequate pulse. When I say claim I don’t mean that I believe the person in this case was lying but rather they believed they felt a pulse. As with many other posts I felt obliged to ask the question “How accurate is assessment of a pulse in a resuscitation?” As much as we would like to think we all stay calm under pressure there is no doubt that when it counts most and our heart is racing from our sympathetic nervous system on overdrive, we may experience the opposite state. A nicely done study addressed such accuracy in 2009 using patients who were on heart lung bypass. 209 doctors and nurses were asked to blindly assess presence or absence of pulse with the manipulation of pulsatility by using the presence of a left ventricular assist device or not. The findings of this study are somewhat disturbing in that 22% of the time they were wrong about the presence of a pulse. In this study they were given as long as they wanted and in no way were under stress to perform. They simply had to say after taking as much time as they needed whether the pulse was present or not. How accurate do you think they would be with a newborn, covered in amniotic fluid and blood with people giving resuscitation orders? Not very accurate I would say.
The NRP program recommends that a rising heart rate is the best indicator of a successful resuscitation. Two hundred years ago a physician brought the stethoscope into our repertoire of tools at our disposal in medicine. Despite all of our focus on non-invasive monitoring during resuscitation, confirmation of a heart rate should only be done by auscultation. Technology serves a useful purpose by providing confirmation of rhythm after hearing the heart beat but should never be used as a substitute for one of the oldest technologies there is.
by All Things Neonatal | Jul 18, 2015 | General Comments
My Call Karma has turned for the worse. At least this is what I told myself as I drove home from the hospital last night. My last seven days has seen me at the deliveries for three infants with a combined weight of 1650g or about 4 lbs and in two other patents lose the battle in our teams fight to preserve a life. There is no doubt this has been trying for myself and for that matter the rest of the teams I have worked with during that time. In the field of Neonatology, members of our team would say this has been “a bad week”. For those that know me you would also say that this is quite surprising as I am known for having good “Call Karma”.
On that 20 minute drive home I had some time to think about that statement and the more I did, the more I questioned (possibly due to a sleep deprived state) why I and other colleagues utter such words. At some point or another I have heard most physicians I know speak in such terms or use the word luck in the place of Karma. What is Call Karma exactly for those of you who are really confused at this point? The concept of Call Karma is that some health care practitioners seem to have very uneventful times when on call and others plagued by the busiest shifts or weeks or service seemingly every time they are working. Before I go on, I will state the obvious, that this seems preposterous to anyone who has read so far and knows anything about statistics unless of course you believe that there are forces at work manipulating probabilities. Nonetheless, if you work in a hospital and listen for it you will hear people mention Call Karma from time to time when things are exceptionally busy or quiet in the NICU while someone is on call or service. This is also not something that is restricted to those with more or less experience, as I have heard it said many times over by people at both ends of the years of service spectrum.
As I was trying to settle myself after a rough night in the NICU I took to several literature search sites and tried to find an article on Call Karma. After spending more time than I would like to admit I came up with zero results. Twitter was more productive, as I came across many tweets on the subject with people referencing both their good and bad experiences in the hospital. What I did not find was a blog post or article on the subject anywhere, yet having worked in two hospitals and heard the expression used countless times it seems it is common vernacular wherever you find health care providers.
What is Karma? Karma as defined by dictionary.com using the Hindu or Buddhist meaning is:
An action, seen as bringing upon oneself inevitable results, good or bad, either in this life or in a reincarnation.
Applying this definition to being on call or service I believe explains exactly what Call Karma is. Women are not choosing when to deliver their infants based on our call schedules nor are babies deciding when and how sick they will get depending on who comes into the NICU that day in their scrubs to start call or service.
Call Karma exists in our heads and is the result of myopic views of our work life combined with confirmation bias and a healthy dose of support from those around us and is inevitable as the definition suggests above for some of us in this life (I will leave the reincarnation piece out of it!). Confirmation bias is the tendency to notice data that confirm our suspicions about the truth as we see it and ignore data streams that contradict that perception. Using the example of call, if five out of ten weeks of service are “busy” and five are more uneventful we will pay no attention to the calm times but accept the label of bad Call Karma when someone mentions it to us during those weeks that are particularly stressful. Myopia rears it’s ugly head in this situation, as we tend to look at the short term events as confirmatory during a bad week rather than remembering the last nine weeks and how they all went as well. We are slaves to the “here and now”.
Finally the last piece of the puzzle has to do with the above definition which includes the words”bringing upon onseself”. How we perceive and handle these busy weeks is just as important as the acuity as observed by others. Are you a health care provider who obsesses over details, likes to micromanage and feels the need to be present in the unit for fear that the people around you can’t be trusted to do as careful a job as you would? If so, your perception of your weeks will be quite different that the practitioner who takes the approach of being more trusting of those on call in the NICU and being more of a big picture person. Our minds can only handle so much information at once and if you have several babies sick at the same time and have a obsessive need to know every sodium, hemoglobin and CRP result trended over time for each patient you will in fact be busier than the person who takes a less micromanaged approach. Same patients, just a different perception of acuity and business and therefore stress. It is such type A behaviour that I believe is what brings most of the karma upon us. It doesn’t take much acuity to have those with such behaviours perceive that they are busier than others. Add to this, people around them who see them in the unit working tirelessly on service and then commenting that their karma is bad and…voila you have the perfect setup for bad Call Karma!
So as I prepare to start this day anew I conclude this post with the following. Call Karma exists but like anything the power to change it lies within yourself. Today may bring good or bad but statistics would say I am due for a break…or not.

by All Things Neonatal | Jul 12, 2015 | General Comments, health care, Neonatal, Neonatology, preemie, Prematurity
Living in Canada we are privileged to have a universal health care system. Privileged in the sense that all citizens are entitled to the same level of care regardless of economic circumstance although the monetary costs to the tax payer is another story and forms the basis of most arguments in the US against adopting such a system down south. My goal of this post though is not to enter into a debate about which system is superior but rather speak of the dollars and cents attributable to being born too early or too small.
In the US such measurements are simpler as costs are more easily measured in a private health care system but each health care region in Canada can measure to a certain degree the costs associated with a hospital stay. Certainly the story of Raquena Thomas made this clear to me. In 2007 she was born in Edmonton after her mother left Jamaica for a visit with family in Edmonton. After delivering she was found to have hypoplastic left heart syndrome (HLHS) and went on to have the first stage of the Norwood procedure. What followed was a bill to the mother for $162576 and for commentary on the discussion that ensued about who should pay the bill see the article here. As I was working at the Stollery Children’s Hospital at the time and cared for this infant it was clear to me after this experience that the hospital indeed has a clear method to calculate costs even if we the taxpayer are blind to such calculations.
Now HLHS is a condition that affects very few infants a year in any given province but what about low birth weight and preterm birth? This as we say in Neonatology is our bread and butter. In 2009 Lim et al published data on the Canadian population in attempt to ascertain the health care costs for these groups of patients (CIHI survey: Hospital costs for preterm and small-for-gestational age babies in Canada)
In this period 1 in 7 babies was born either preterm or small for gestational age. If specifically looking at infants < 2500g defined as low birth weight this represented 6% of all babies born. When you factor in that there were 350000 babies born in that year in Canada we are looking at about 21000 babies nationally. 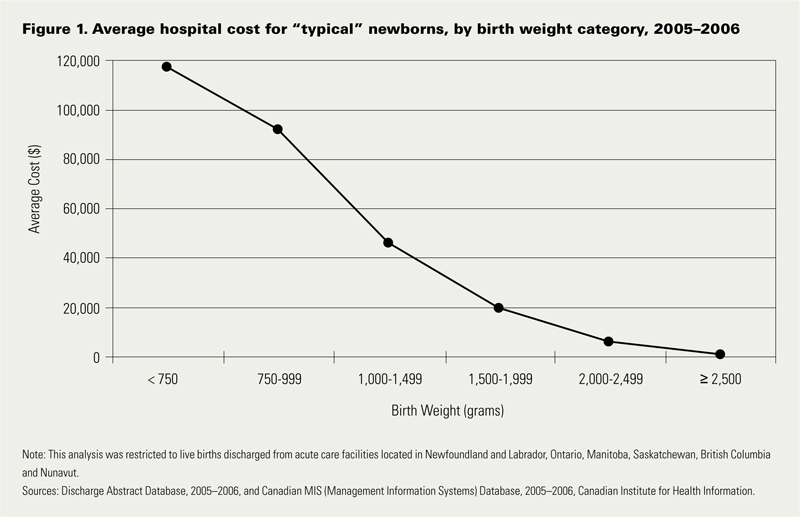 Looking at the costs for these infants one sees a direct relationship between decreasing birth weight and increasing costs in the hospital. This should not be surprising to anyone. It should be noted though that the paper provides average costs only without standard deviation or ranges. As you would expect, the costs for a patient with severe HIE or NEC would be higher than the 26 week infant who has a very smooth course and does not have a symptomatic PDA, severe IVH or any other significant disability during their course.
Looking at the costs for these infants one sees a direct relationship between decreasing birth weight and increasing costs in the hospital. This should not be surprising to anyone. It should be noted though that the paper provides average costs only without standard deviation or ranges. As you would expect, the costs for a patient with severe HIE or NEC would be higher than the 26 week infant who has a very smooth course and does not have a symptomatic PDA, severe IVH or any other significant disability during their course.
The data looking at such costs is scare with respect to the Canadian landscape and even more difficult to determine has been lifetime costs or at least incremental costs after leaving the hospital environment. I was delighted to see that former colleagues of mine in Edmonton have published a new paper examining both the extent of health service utilization (HSU) attributable costs in the year following discharge of both LBW and normal birth weight peers in Alberta (abstract here). Not surprisingly, smaller babies have more medical needs. In this study LBW patients had an average of 5.9 outpatient services and 1.1 visits to the ER in the first year of life compared to 2 and 0.9 in the normal birth weight peers. Physician services were double with 22.7 office visits compared to 11.9 in the NBW group. The costs to the Health Care system overall are represented in the table below which demonstrates that the LBW infants make up 37% of the total health care costs of newborns yet represent only 6% of the population. In terms of risk factors for LBW they were high prepregnancy weight, aboriginal women and low socioeconomic status. Efforts to lessen the incidence of the first and third factor in our pregnant population would be a good target for public health efforts. Bear in mind that the costs outlined below are in addition to the costs in the hospital.
| BW Category |
Cost per patient |
Patients |
Cost to System (millions) |
| NBW |
$3,942 |
43207 |
182 |
| LBW <2500 |
$33,096 |
3123 |
108 |
| 1500 – 2499g (MLBW) |
$20,467 |
2571 |
53 |
| 1000 – 1499g (VLBW) |
$83,895 |
278 |
23 |
| < 1000g (ELBW) |
$117,546 |
274 |
32 |
The analysis provided in this paper does not specify out the costs by certain conditions such as NEC or BPD so all we have to go on are averages for HSU and cost. It does however raise a point which I believe is crucial to any discussions with respect to expanding programs within the hospital. We need to refocus administration at both the hospital level and at the funding source (our provincial governments) as to the true costs of the conditions that we are trying to prevent. It is only through looking at the costs of both the hospitalization and after discharge that we can truly come to understand the cost effectiveness of expanded programs or new treatment modalities.
Donor breast milk is one that I believe serves as a good example of a program that is in need of expansion in many places in the country but is hampered by the perception of high up front costs. The average cost of this milk is about $4 per ounce. I will simplify the math a little as there would be a phase of escalating the volume per day and a wean at the end but let’s say we have a 1.5 kg infant that we want to treat with DBM for a period of 4 weeks. The cost to do this assuming a TFI of 150 mL/kg/d would be a little over $800 per patient so with the increasing phase, wean and adjusting for some weight gain let’s say $1000 per patient. If there were 200 such patients in your hospital each year the annual cost would be $200000 which on the surface seems like a lot of money. From the most recent cochrane review though comparing formula to donor milk the risk ratio to develop NEC is 2.77 meaning that a preterm baby who receives formula is nearly three times as likely to develop NEC. Ignoring differing rates of NEC by hospital let’s just use the concept that we could prevent one case of NEC a year with such a strategy. The cost of medical NEC is somewhere between 100-140K while surgical is 200 – 240K. The in-hospital costs of preventing just one case nearly pay for or exceed the cost of the entire years supply of DBM. If you add to this the cost of the following years of physician visits, consultants, testing, special diets and investigations and procedures these patients receive the costs are more than covered from just one patient.
Health care budgets are no doubt a difficult thing to balance but the point of all of this is that when determining whether to spend our precious health care dollars we must look at not only the impact during the hospitalization but for years after if we truly modify future risks as well.
