

On occasion two articles will be published in short succession and have discrepant findings. This appears to be one of those times. Hishikawa K in Japan published a paper in September entitled Pulmonary air leak associated with CPAP at term birth resuscitation while Calebi MY from Turkey published Impact of Prophylactic Continuous Positive Airway Pressure on Transient Tachypnea of the Newborn and Neonatal Intensive Care Admission in Newborns Delivered by Elective Cesarean Section in August of this year.
The findings as we will discuss were quite discrepant which on the surface leaves the practitioner in a quandry. How do I best treat my patients? The key difference between the two studies was the finding of an increased rate of pneumothorax in the study by Hishikawa when CPAP was used in term infants with respiratory distress after delivery. Curiously prophylactic CPAP of +5 was used in both studies but the populations under study were quite different. The study by Calebi targeted infants between 34 0/7 weeks and 38/6/7 weeks vs term infants in the study from the Japanese group.
Another important difference is the utilization of CPAP which in the study by Calebi involved prophylactic administration within twenty minutes of birth and in the Japanese cohort the indication was the development of symptoms. Thinking about this for a moment, these two groups are actually quite different. A newborn with TTN has an increased amount of interstitial fluid that has not made it’s way to the hilum for reabsorption in the lymphatic system. The lungs of these infants are heavier with fluid than comparable infants without such pathology and therefore are also less compliant. Non compliant lungs are prone to microatelectasis as the infants progressively experience alveolar collapse. The longer the clinician waits to start supportive CPAP the more the lungs collapse and greater negative pressure is required to open these closing alveoli. Furthermore if there is fluid in the airway itself there is the potential for a ball valve mechanism to come into effect whereby air is able to pass through the dilated airways during inspiration but on expiration the collapse leads to air trapping. Such trapping places the infant at risk for air leak. CPAP is used to establish an adequate functional residual capacity (FRC) as indicated in this picture. 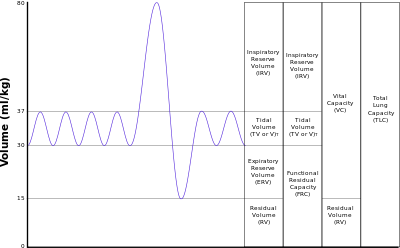 Failure to do so results in atelectasis.
Failure to do so results in atelectasis.
The Japanese study examines the impact of CPAP after a change in guidelines in 2010 suggesting that CPAP should be utilized in the delivery suite for those infants with ongoing respiratory distress. The study by Calebi really examines a different patient group being those who are near term patients with TTN who have early CPAP implemented. The early administration of CPAP may be the technique that prevents alveolar collapse as mentioned above and avoids the requirement by the infant to generate such high negative pressure with its inherent risk of air leak.
Is All CPAP The Same?
Another important distinction between the two papers is the way in which CPAP was administered. The Japanese utilized a flow inflating bag with a pressure valve and manometer while the study by Calebi employed a T-piece resuscitator. When it comes to maintaining CPAP there is no question having used both devices that I find the T-piece resuscitator much easier to use and over longer periods the reliability of the pressure delivered by the T-piece would be superior to that with the flow inflating bag. The Neopuff T-Piece Resuscitator possesses a pressure relief valve which could help during an instance when the patient is crying or breath holding. The constant flow without a relief valve could lead to airleak which is precisely the situation that may occur during the use of a flow inflating bag.
Yes there was over a three fold increase in airleak at near term gestational age in the Japanese cohort but this was not seen at all in the Turkish study in which CPAP was implemented early. So the message here is that if you start CPAP early enough you can prevent airleaks from occurring. This in and of itself is worth implementing.
Can CPAP Reduce Hospital Admission to NICU?
There is more to the story however. The Turkish group demonstrated a significant difference in admission rates to the NICU as shown in the following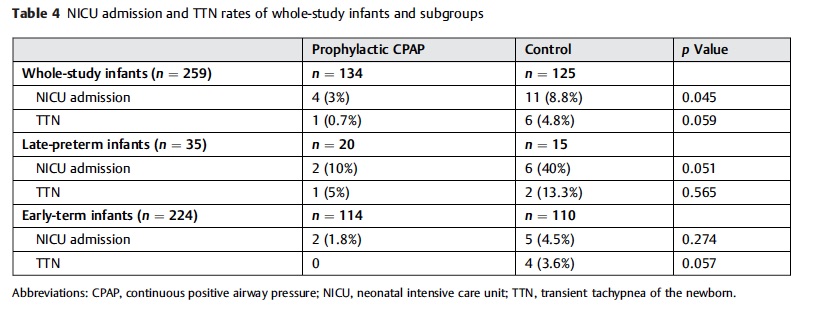 figure. The results here although just achieving significance should not be minimized. Avoiding progressive atelectasis decreases admission rates. The conclusion here is that there is little benefit in adopting a wait and see approach to those kids born by elective c-section. While it is true that you may be treating a significant number of healthy patients between 34 0/7 – 38 6/7 weeks with CPAP it is for a brief period and makes a significant difference in frequency of admission.
figure. The results here although just achieving significance should not be minimized. Avoiding progressive atelectasis decreases admission rates. The conclusion here is that there is little benefit in adopting a wait and see approach to those kids born by elective c-section. While it is true that you may be treating a significant number of healthy patients between 34 0/7 – 38 6/7 weeks with CPAP it is for a brief period and makes a significant difference in frequency of admission.
We live in an era of bed shortages and I would argue that anything we can do to reduce admissions and moreover keep babies with their parents is worth exploring. From my perspective treating these kids with the appropriate CPAP device for twenty minutes after birth is well worth it. Perhaps your unit should consider the same.
Hi Michael, I’m curious as to why NRP is so against cpap in the term infant given your take on these studies? My understanding has been that it’s the risk of pneumothorax along with a general lack of evidence, not so much that there is evidence against it. Our physicians are quick to use cpap with any post delivery respiratory distress, but there are other practitioners in the province who are very against it and abide by NRP’s approach with only moderate+ distress. This delayed (NRP)approach seems to be less effective if I’m understanding your article.
Thoughts?
Just took the 7ed NRP. Didn’t notice them specify not to use CPAP in term babies. Would not delay the use of CPAP in any baby with respiratory distress. An x-ray or ultrasound if available may be very helpful though in ruling out a pneumo as a cause of the distress as well. Do you have a section of the textbook though that specifically singles out term infants as ones who should not get CPAP?
Missed this in October….
I worry that early CPAP would have the opposite effect from what you suggest by separating more babies and parents. Most smaller units would be admitting (at least for a short period of observation) any baby that needed CPAP in the delivery suite.
Erik thank you for commenting. I see it as something that yes will disrupt infant/maternal bonding for a few but for more will prevent the longer separation if you allow their lungs to slowly collapse. The Turkish study I quoted noted a reduction in admission rates with use of early CPAP. I would say that this has been our experience here as well in that some patients who need CPAP early are off by a few hours and then off to their families. If you were to delay and they developed significant atelectasis you would be playing catch up and need longer times on the devices