
by All Things Neonatal | Apr 27, 2016 | Infection, reflux, Uncategorized
Preamble
May 7, 2017
As I sit drinking my morning coffee and feeling a little sense of heartburn I began to reflect on the fact that I can’t recall the last time I prescribed ranitidine or a PPI in an infant for anything other than an acute upper GI bleed. I know I had done so after moving to Winnipeg in 2010 at a few time points but that practice has certainly died at least for me. You know what? I don’t think it has made one iota of difference but based on the results from this post I think it is for the best. What has inspired my republishing of this post is my question as to whether or not you think your units practice has changed as well since the revelation that these medications are not only ineffective but harmful. Read on and enjoy your Sunday
Choosing wisely is an initiative to “identify tests or procedures commonly used whose necessity should be questioned and discussed with patients. The goal of the campaign is to reduce waste in the health care system and avoid risks associated with unnecessary treatment.”
The AAP Section on Perinatal Pediatrics puts the following forth as one of their recommendations.
“Avoid routine use of anti-reflux medications for treatment of symptomatic gastroesophageal reflux disease (GERD) or for treatment of apnea and desaturation in preterm infants.
Gastroesophageal reflux is normal in infants. There is minimal evidence that reflux causes apnea and desaturation. Similarly, there is little scientific support for the use of H2 antagonists, proton-pump inhibitors, and motility agents for the treatment of symptomatic reflux. Importantly, several studies show that their use may have adverse physiologic effects as well as an association with necrotizing enterocolitis, infection and, possibly, intraventricular hemorrhage and mortality.”
How strong is the evidence?
The evidence for risk with acid suppression is largely based on either retrospective or in the case of Terrin G et al a prospective observational cohort study Ranitidine is Associated With Infections, Necrotizing Enterocolitis, and Fatal Outcome in Newborns. In this study the authors compared a group of premature infants with birth weights between 401 – 1500g or 24 – 32 weeks gestation who received ranitidine for reflux symptoms to those who did not. All told 91 were exposed while 183 were not. The authors are to be commended for standardizing the feeding protocol in the study so that when comparing NEC between groups one could not blame differences in formula consumption or rate of feeding advancement. Additionally, bias was controlled by having those not involved in care collect outcome data without knowing the purpose of the study. Having said that, they may have been able to ascertain that ranitidine was used and have been influenced in their assessments.
The patients in terms of risk factors for poor outcome including CRIB and apgar scores, PDA etc were no different to explain an increased risk for adverse outcome.
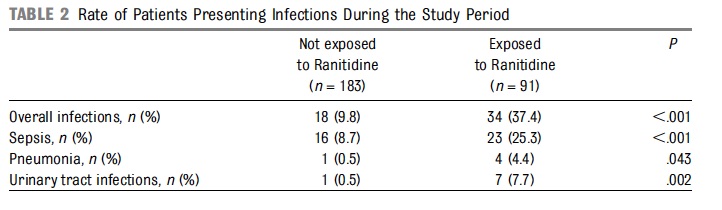
From the above table, rates of infections were clearly higher in the ranitidine group but more concerning was the higher rate of mortality at 9.9% vs 1.6% P=0.003 and longer hospitalization median 52 vs 36 days P=0.001.
Results of a Meta-Analysis
Additional, evidence suggesting harm comes from a meta-analysis on the topic by More K, Association of Inhibitors of Gastric Acid Secretion and Higher Incidence of Necrotizing Enterocolitis in Preterm Very Low-Birth-Weight Infants. This analysis actually includes the study by Terrin and only one other retrospective database study of 11072 patients by Guillet et al. As the reviewers point out the study by Terrin while prospective did not employ the use of multiple regression to adjust for confounders while the larger study here did. In the end the risk of NEC with the use of acid suppression was 1.78 (1.4 – 2.27; p<0.00001).
What do we do with such evidence?
I can say this much. Although small in number, the studies that are available will make it very difficult to ever have a gold standard RCT done on this topic. This scant amount of evidence, backed by the biologic plausibility that raising the gastric pH will lead to bacterial overgrowth and potential aspiration of such contents provides the support for the Choosing Wisely position.
Why do we continue to see use of such medications though? It is human nature I suspect that is the strongest motivator. We care for infants and want to do our best to help them through their journey in neonatal units. When we hear on rounds that the baby is “refluxing” which may be documented by gulping during a brady, visible spit ups during A&Bs or through auscultation hearing the contents in the pharynx we feel the need to do something. The question invariably will be asked whether at the bedside or by the parents “Isn’t there something we can do?”.
My answer to this is yes. Wait for it to resolve on its own, especially when the premature infants are nowhere close to term. I am not sure that there is any strong evidence to suggest treatment of reflux episodes with gastric acid suppression helps any outcomes at all and as we see from the Terrin study length of stay may be prolonged. I am all in favour of positional changes to reduce such events but with respect to medications I would suggest we all sit on our hands and avoid writing the order for acid suppression. Failure to do so will likely result in our hands being very busy for some infants as we write orders to manage NEC, pneumonia and bouts of sepsis.

by All Things Neonatal | Apr 20, 2016 | jaundice, Uncategorized
As the saying goes “What is old is new again” and that may be applicable here when talking about prevention of kernicterus. In the 1990s there was a great interest in a class of drugs called mesoporphyrins in the management of hyperbilirubinemia. The focus of treatment for many years had been elimination of bilirubin through the use of phototherapy but this shifted with the recognition that one could work on the other side of the equation. That is to prevent the production of bilirubin in the first place.
Tin mesoporphyrins (SnMP) have the characteristic of being able to inhibit the enzyme hemo oxygenase quite effectively. 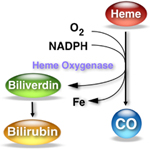 By achieving such blockade the breakdown of heme to carbon monoxide and biliverdin (the precursor of bilirubin) is inhibited. In so doing, the production of bilirubin is reduced making one less dependent on phototherapy to rid the body of elevated levels. So simple and as you might imagine a good reason for there to have been significant interest in the product. One article by Martinez et al entitled Control of severe hyperbilirubinemia in full-term newborns with the inhibitor of bilirubin production Sn-mesoporphyrin. was published in 1999 and demonstrated that infants with severe hyperbilirubinemia between 48-96 hours could have their need for phototherapy eliminated by use of the product compared to 27% of the infants in the control group needing treatment. Additionally, total bilirubin samples were reduced from a median of 5 to 3 with the use of one IM injection of SnMP. This small study was hampered though by inability to really look at adverse outcomes despite its effectiveness. What has been seen however is that SnMP if given to infants who are then treated with white lights can create a rash which is not seen however when special blue light is employed.
By achieving such blockade the breakdown of heme to carbon monoxide and biliverdin (the precursor of bilirubin) is inhibited. In so doing, the production of bilirubin is reduced making one less dependent on phototherapy to rid the body of elevated levels. So simple and as you might imagine a good reason for there to have been significant interest in the product. One article by Martinez et al entitled Control of severe hyperbilirubinemia in full-term newborns with the inhibitor of bilirubin production Sn-mesoporphyrin. was published in 1999 and demonstrated that infants with severe hyperbilirubinemia between 48-96 hours could have their need for phototherapy eliminated by use of the product compared to 27% of the infants in the control group needing treatment. Additionally, total bilirubin samples were reduced from a median of 5 to 3 with the use of one IM injection of SnMP. This small study was hampered though by inability to really look at adverse outcomes despite its effectiveness. What has been seen however is that SnMP if given to infants who are then treated with white lights can create a rash which is not seen however when special blue light is employed.
Two other studies followed exploring the use of SnMP in cases of severe hyperbilirubinemia in term infants and were the subject of a Cochrane review in 2003. The conclusions of the review essentially became the death nell for the therapy as they were as follows.
“…may reduce neonatal bilirubin levels and decrease the need for phototherapy and hospitalization. There is no evidence to support or refute the possibility that treatment with a metalloporphyrin decreases the risk of neonatal kernicterus or of long-term neurodevelopmental impairment due to bilirubin encephalopathy… Routine treatment of neonatal unconjugated hyperbilirubinemia with a metalloporphyrin cannot be recommended at present.”
The literature after this basically dries up, that is until this month when a paper emerges that is best described as a story of mystery and intrigue!
Prophylactic Use of SnMP From 2003 Published in 2016!
This paper as you read it almost seems like a conspiracy story. The paper is by Bhutani et al (as in the nomogram) Clinical trial of tin mesoporphyrin to prevent neonatal hyperbilirubinemia. The study set out to answer a different question than had been previously studied. The question here was, if you provided a single IM dose of SnMP to infants who were at or above the 75%ile on the risk nomogram, could you prevent the need for phototherapy or exchange transfusion as the primary outcome. Secondarily, the authors truly wanted to demonstrate safety of the product and planned on recruiting 800 patients per arm in the study. The study appeared to be well planned and as with many studies had a safety monitoring committee which was to do interim analyses. After the first analysis the FDA became involved and recommended studies to look at a prophylactic versus therapeutic approach. Due to the interim analysis the study had been halted and after the FDA made their suggestion the study was simply never restarted as future studies were planned to look at the effectiveness and safety of the two approaches. The authors state that they planned on reporting their results in 2006/7 but elected to wait until long term data emerged. Now finally 9 years later they decided to release the results of the partially completed study. The story around this study I find as interesting as the results they obtained!
So What Happened?
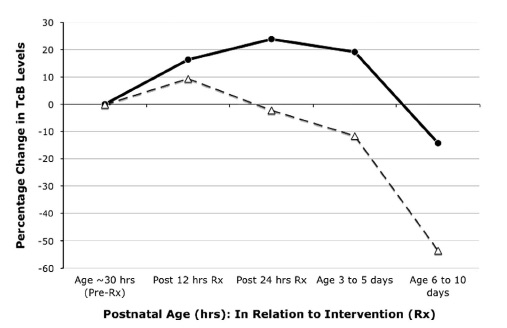
Before closing the study they managed to recruit 87 into the intervention arm and 89 into the placebo group and lost none to follow-up. One dose of SnMP had a significant effect on the trajectory of curves for bilirubin production as can be seen in the first figure.
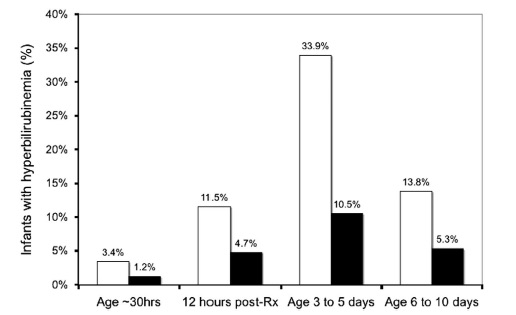
The graph below demonstrates what percentage of patients had a bilirubin level above 220 umol/L (12.9 mg/dl) after the single injection of SnMP (black bars) compared to placebo (white bars).
What can we do with these results?
It would be tough to argue anything other than this being an effective treatment to prevent significant hyperbilirubinemia. Unfortunately, like many studies that were never completed this one remains underpowered to conclusively demonstrate that the use of SnMP is safe in both the short and long term periods. The absence of such data make it very difficult to recommend SnMP as standard of care. One has to add to this that while we have evidence to show it reduces the rate of rise of bilirubin, what we don’t know is whether in a larger study the incidence of bilirubins > 425 umol/L or the need for exchange transfusion might be reduced. If this were the case, it would make for a compelling argument to try SnMP.
That is the approach for standard of care though. In the setting of a patient with a known blood group incompatibility who was at high risk for exchange transfusion, if they received IVIG and the bilirubin continued to climb might there be a role here? I would tend to say yes if we could get our hands on some. The authors by sharing this data have shown the medication is effective in doing what it is supposed to do. Given that at least in our centre all of our lights are of the new variety, the risk of rash would be nonexistent. The risk for kernicterus or at least an exchange transfusion though would not be minimal so if we have this in our toolbox I would after weighing the risks opt to give it.
I certainly wonder if there are places out there who have used it and if so what is your experience?

by All Things Neonatal | Apr 15, 2016 | kangaroo care
After releasing yesterdays post Skin to Skin Fad Blamed For Death of Babies I entered into a very interesting discussion on Twitter with Clay Jones of Science Based Medicine.org. Emily Hahn (@TexasKidDoc) was also instrumental for setting up the discussion so I thank her for connecting Clay and I once again. At issue was whether the “Fad” of Skin to Skin Care was indeed to blame for the observations in Australia.
Clay in fact his written on this topic as well but from KC in the term infant perspective and I would encourage you to read his piece as a “counterpoint” below.
My gut reaction given that I am immersed in a culture of Kangaroo Care was to defend the usage but he raises a very important point that I think is worth addressing.
No one is disputing the benefits of Kangaroo Care for preterm infants which I won’t go into here as I have done so yesterday. The question being posed is whether such benefits extend to the term infant and whether it can be done safely. The preterm infant experiencing KC in a prone position is of course monitored with a nurse close by. The patient in the room alone with a mother who has recently delivered is not necessarily supervised to the same degree. Also if the baby is unmonitored then is it safe?
Still A Big Supporter of Kangaroo Care
I am not changing my tune so to speak as there are many benefits in terms of breastfeeding, maternal-infant bonding, thermoregulation etc that will be achieved through KC. What I do mean to at least raise some awareness of though is the concern that without a proper preventative strategy in the term infant population falls and or asphyxiation from a mother who falls asleep with the infant in between her breasts is possible. Readers of this blog on Facebook yesterday acknowledged they have seen such events happen and I can say myself that I have as well.
Let’s practice KC and endorse it but in the end let’s all be safe. In the end the question then is was the title of the Yahoo post truly that inflammatory?! What it inferred I think was but as it pertained to the hospital experience perhaps there was something there.
What do you think?
Addendum: From Keith Barrington
There are now several publications about this happening, (including our case report, Schrewe B, et al. Life-threatening event during skin-to-skin contact in the delivery room. BMJ Case Rep. 2010;2010(dec21 1):bcr1120103475-bcr.) At the time we wrote our report we found 59 cases in the literature, and 56 of them had been in skin to skin with the mother.
A French group published a number of risk factors for sudden unexpected life-threatening events after an uneventful delivery at term, which included skin to skin position and maternal obesity.
It is clear that this is very rare ( German group calculated the incidence as 2.6 per 100,000 deliveries), but it is potentially devastating, mortality is high, and neurologic compromise also.
Our take on this was that given the benefit in terms of breast feeding initiation etc, and the rarity of problems, that we should not discourage the practice, but never leave a new mother alone with the baby in skin to skin, someone else should be in the room to keep an unobtrusive eye on the baby, it could be the father (if he had some idea what to watch for) or a health care worker. As the mechanism is probably simple suffocation, a pulse oximeter could be a potential way of surveying for teh occurrence, if something more natural was not available.

by All Things Neonatal | Apr 14, 2016 | kangaroo care
As the practice seems to be winning the world over you can imagine that a headline entitled,
would get some attention. This article was sent to me by a colleague after being published last month on Yahoo news service. The claim is based on the experience of a hospital in Perth that has seen some cases of neonatal suffocation after mothers who were performing skin to skin care fell asleep and rolled onto their newborn. This “fad” they say is attributable as the cause of death. Before looking into whether there is any basis for such a claim it may be worth exploring whether Kangaroo Care (KC) otherwise known as Skin to Skin (STS) care is effective. The irony is not lost on me either that safety of Kangaroo Care is being challenged in Australia…
Is KC Effective in the NICU?
KC or is an ideal method of involving parents in the care of their premature infant. It fosters bonding between parents and their hospitalized infant, encourages the family to be with their child and thereby exposes them to other elements of neonatal care that they can take part in.
Before you reach the conclusion that KC only serves to enhance the parental experience it does so much more than that. The practice began in Bogota Columbia in 1979 in order to deal with a shortage of incubators and associated rampant hospital infections. The results of their intervention were dramatic and lead to the spread of this strategy worldwide. The person credited with helping to spread the word and establish KC as a standard of care in many NICUs is Nils Bergman and his story and commentary can be found here.
The effects of KC are dramatic and effective to reduce many important morbidities and conclusively has led to a reduction in death arguably the most important outcome. An analysis of effect has been the subject of several Cochrane Collaboration reviews with the most recent one being found here.
To summarize though, the use of KC or STS care has resulted in the following overall benefits to premature infants at discharge or 40 – 41 weeks’ postmenstrual age:
Reduction in
mortality (typical RR 0.68, 95% CI 0.48 to 0.96)
nosocomial infection/sepsis (typical RR 0.57, 95% CI 0.40 to 0.80)
hypothermia (typical RR 0.23, 95% CI 0.10 to 0.55)
Increase in
KMC was found to increase some measures of infant growth, breastfeeding, and mother-infant attachment
To put this in perspective, medicine is littered with great medications that never achieved such impact as simply putting your child against your chest. This is another shining example of doing more with less. This is not to say that modern medicine and technology does not have its place in the NICU but KC is simply too powerful a strategy not to use and promote routinely in the NICU.
What About Term Infants?
Much has been written on the subject. A Pilot study in 2007 by Walters et al found benefits in newborn temperature, glycemic control and initiation of breastfeeding. Perhaps the strongest evidence for benefit comes from a cochrane review of the subject last updated in 2012.
This analysis included 34 RCTs with 2177 participants (mother-infant dyads). Breastfeeding at one to four months postbirth (13 trials; 702 participants) (risk ratio (RR) 1.27, 95% confidence interval (CI) 1.06 to 1.53, and SSC increased breastfeeding duration (seven trials; 324 participants) (mean difference (MD) 42.55 days, 95% CI -1.69 to 86.79) but the results did not quite reach statistical significance (P = 0.06). Late preterm infants had better cardio-respiratory stability with early SSC (one trial; 31 participants) (MD 2.88, 95% CI 0.53 to 5.23). Blood glucose 75 to 90 minutes following the birth was significantly higher in SSC infants (two trials, 94 infants) (MD 10.56 mg/dL, 95% CI 8.40 to 12.72).
Taken together there are benefits although the impact on breastfeeding rates in term infants show a strong trend while not reaching statistical significance. Importantly though in this large sample we don’t see any increase in mortality nor to my knowledge has there ever been a study to show an increase.
How do we deal with this claim from Australia then?
I think the problem with this claim is that KC is being blamed after a “root cause analysis” has come to the wrong conclusion. The problem is not KC but rather a lack of a “falls prevention” strategy on the postpartum units. Mothers after delivery are exhausted and may be on pain medication so as the saying goes “there is a time and a place”. As our hospital prepares for accreditation again, safety to prevent falls (including babies falling out of mom’s arms or in a similar vein mothers falling onto babies) is something that every hospital needs. Whether a mother is practicing KC, breastfeeding or simply holding her baby if a mother falls asleep while doing so there is a risk to the infant. If the hospital in this case has seen an increase in such cases of newborn deaths while performing KC then it is likely the hospitals lack of attention to minimizing risk in the postpartum period that is to blame and not KC itself. Certainly the evidence from rigorously done trials would not support this claim.
This hospital would do well to have a comprehensive plan to educate parents about the risks of fatigue, ensure bassinets are next to every bed to provide mothers with an easy transfer if they are tired. Certainly during the immediate period after delivery mothers, partners of mothers who have just delivered should be encouraged to be with them or advise the mothers if they are tired to put the baby down and rest. A little education could go a long way!
I think it is a cheap out to blame KC for such problems as it turns our attention away from the real issue and that is a lack of policy and education. So in the end I would like to state emphatically that…
No I don’t believe the “skin-to-skin fad” is to blame for an increase in deaths!

by All Things Neonatal | Apr 8, 2016 | preemie, Uncategorized
It seems the expression “(insert a group) lives matter” is present everywhere these days so I thought I would join in after a moving experience I had today. For those of you who have been with the blog since the beginning you would have seen a number of posts that if you follow them in time, provide a glimpse into the transformation that Winnipeg has seen over the last year or so.
Prior to that point, 24 weeks was a cutoff for resuscitation that had been in place for some time and after a great amount of deliberation and thought was changed to 23 weeks. This did not come without a great deal of angst and a tremendous amount of education and teamwork that our nurse educators and clinical leads were so instrumental in helping to role out. The experience was outlined in a couple of posts that you may find interesting if you didn’t catch them the first time. The first was Winnipeg hospital now resuscitating all infants at 22 weeks! A media led case of broken telephone. and the second being Winnipeg Hospital About to Start Resuscitating Infants at 23 weeks!
Since these two posts we have certainly had our fair share of experience as we have seen far more babies than anticipated but the region has met the challenge head on and although the numbers are small we appear to have not only more survivors than expected but all but one infant had gone home without O2 and all have been demand feeding at discharge. While we await the 18 month outcomes, the results thus far appear reassuring.
A Special & Memorable Visit
Then today, a visit occurred from the first of such infants who is now just over a year of age. He was bright eyed, smiling, interactive and by his parent’s account, has normal tone and assessments thus far by physiotherapy. His presence in the NICU put smiles on faces and at least for myself made me think of the expression “Micropreemie Lives Matter”. He was a baby that everyone predicted would not survive and then when he did, that he would be grossly developmentally impaired which he does not appear to be in the least. His presence in the unit no doubt gives everyone who doubted the merits of moving down this path reason to pause.
Before you accuse me of wearing rose coloured glasses, make no mistake I know that he will not represent the outcome for everyone. In fact at one of our hospitals two of such infants have died while we await the 18 month outcomes for the other survivors. What his presence does though, is remind us or at least me that good outcomes are possible and in the case of our experience in Winnipeg may be more common that we thought they would be.
Black Swans and Human Nature
When I have spoken to audiences about the path forward when resuscitating such ELGANS I have often commented on the “Black Swan” effect.  This was very nicely described by Nassim Taleb and described the human trait to react to unusual events with extreme reactions. An example is no one wanting to fly in the months after the world trade centre bombing when statistically this may have been the safest period in history to fly. Similarly, we as a team need to avoid the extreme reaction of saying that we should not be resuscitating such small infants when a bad outcome occurs. As I have told many people, we know these patients will not all survive, we know a significant number will have adverse development yet not all will and at least in our small sample thus far the babies would appear to be doing better overall than anticipated. If we know that bad outcomes will occur then why do we hear the questions come when they do such as “why are we doing this?”, “maybe we should rethink our position on 23 week infants”. It happens because we care and we hate seeing families and their babies go through such painful experiences. What we cannot do though for the sake of those such as our visitor today is react with a “Black Swan” reaction and steer the ship so to speak in the previous direction we were in. There are survivors and they may do well and that is why I say “Micropreemie Lives Matter”.
This was very nicely described by Nassim Taleb and described the human trait to react to unusual events with extreme reactions. An example is no one wanting to fly in the months after the world trade centre bombing when statistically this may have been the safest period in history to fly. Similarly, we as a team need to avoid the extreme reaction of saying that we should not be resuscitating such small infants when a bad outcome occurs. As I have told many people, we know these patients will not all survive, we know a significant number will have adverse development yet not all will and at least in our small sample thus far the babies would appear to be doing better overall than anticipated. If we know that bad outcomes will occur then why do we hear the questions come when they do such as “why are we doing this?”, “maybe we should rethink our position on 23 week infants”. It happens because we care and we hate seeing families and their babies go through such painful experiences. What we cannot do though for the sake of those such as our visitor today is react with a “Black Swan” reaction and steer the ship so to speak in the previous direction we were in. There are survivors and they may do well and that is why I say “Micropreemie Lives Matter”.
In the paper by Rysavy the overall finding at 23 weeks was that 1 out of 6 would survive without moderate or severe disability. What do we do as we increase our experience if the trend bears out that our outcomes are better? How will we counsel families? Will we continue to use the statistics from the paper or quote our own despite us being a medium sized centre?
The Big Questions
As our experience with such infants increases we will also no doubt see a change in our thoughts about infants at 24 weeks. I have seen this first hand already with a physician commenting today that 24 weeks is not such a big deal now! This brings me to the big question (which I will credit a nurse I work with for planting in my head in the last two weeks) which is for another time to answer as this post gets a little lengthy but is something to ponder. As our outcomes for 23 weeks improve and so do our results at 24 weeks (which is bound to happen with the more frequent team work in such situations) will our approach to infants at 24 weeks change. In our institution we generally follow the CPS guidelines for the management of infants at extremely low GA and offer the choice of resuscitation at 24 weeks. As outcomes improve at this GA will we continue to do so or will we reach a threshold where much like the case at 25 weeks we inform families that we will resuscitate their infant without providing the option of compassionate care?
It is too early to answer these questions conclusively but they are very deserving of some thought. Lastly, I would like to thank the parent who came by today for inspiring me and to all those who will follow afterwards.
