

I had a chance recently to drive a Tesla Model S with autopilot. Taking the car out on a fairly deserted road near my home I flicked the lever twice to activate the autopilot feature and put my hands behind my head while the vehicle took me where I wanted to go.  As I cruised down the road with the wheel automatically turning with the curves in the road and the car speeding up or slowing down based on traffic and speed limit notices I couldn’t help but think of how such technology could be applied to medicine. How far away could the self driving ventilator or CPAP device be from development?
As I cruised down the road with the wheel automatically turning with the curves in the road and the car speeding up or slowing down based on traffic and speed limit notices I couldn’t help but think of how such technology could be applied to medicine. How far away could the self driving ventilator or CPAP device be from development?
I have written about automatic saturation adjustments in a previous post but this referred to those patients on mechanical ventilation. Automatic adjustments of FiO2. Ready for prime time? Why is this goal so important to attain? The reasoning lies in the current design trends in modern NICUs. We are in the middle of a large movement towards single patient room NICUs which have many benefits such as privacy which may lead to enhanced breastfeeding rates and increased parental visitation. The downside, having spoken to people in centres where such designs are already in place is the challenge nursing faces when given multiple assignments of babies on O2. If you have to go from room to room and a baby is known to be labile in their O2 saturations it is human nature to turn the O2 up a little more than you otherwise would to give yourself a “cushion” while you are out of the room. I really don’t fault people in this circumstance but it does pose the question as to whether in a few years we will see a rise in oxygen related tissue injury such as CLD or ROP from such practice. In the previous post I wrote about babies who are ventilated but these infants will often be one to one nursed so the tendency to overshoot the O2 requirements may be less than the baby on non- invasive ventilation.
A System For Controlling O2 Automatically For Infants on Non-Invasive Ventilation
This month in Archives Dr. Dargaville and colleagues in Australia provide two papers, the first demonstrating the validation of the mathematical algorithm that they developed to control O2 and the second a clinical report outlining how well the system actually performed on patients. The theoretical paper Development and preclinical testing of an adaptive algorithm for automated control of inspired oxygen in the preterm infant. is a challenge to comprehend although validates the approach in the end while the clinical paper at least for me was easier to digest Clinical evaluation of a novel adaptive algorithm for automated control of oxygen therapy in preterm infants on non-invasive respiratory support.
The study was really a proof of concept with 20 preterm infants (mean GA 27.5 weeks, 8 days of age on average) included who each underwent two hours of manual control by nursing to keep saturations between 90-94% and then 4 hours of automated control (sats 91 – 95%) then back to manual for two hours. The slightly shifted ranges were required due to the way in which midpoint saturations are calculated. The essential setup was a computer equipped with an algorithm to make adjustments in FiO2 using an output to a motor that would adjust the O2 blender and then feedback from an O2 saturation monitor back to the computer. The system was equipped with an override to allow nursing to adjust in the event of poor signal or lack of response to the automatic adjustment.
The results though demonstrate that the system works and moreover does a very good job! The average percentage of time that the saturations were in the target range were significantly better with automated control (81% automated, 56% manual). As well as depicted in the following figure the amount of time spent in both hypoxic and hyperoxic ranges was considerable with manual control but non-existent on either tail with automated control (defined as < 85% or > 98% where black bars are manual control and white automatic).
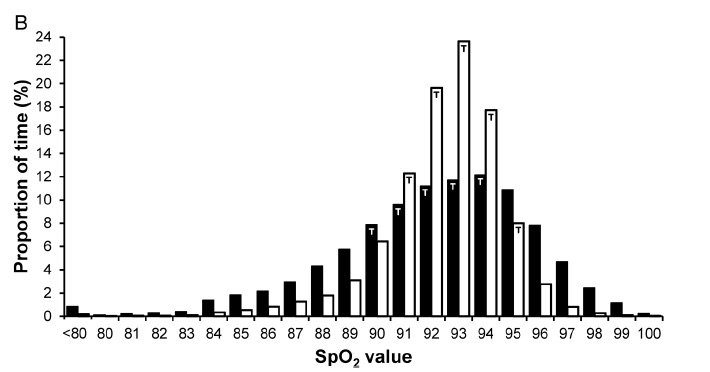
From the figure you can see that the amount of time the patients are in target range are much higher with automatic control but is this simply because in addition to automatic control, nurses are “grabbing the wheel” and augmenting the system here? Not at all.
“During manual control epochs, FiO2 adjustments of at least 1% were made 2.3 (1.3–3.4) times/hour by bedside staff. During automated control, the minimum alteration to FiO2 of 0.5% was being actuated by the servomotor frequently (9.9 alterations/min overall), and changes to measured FiO2 of at least 1% occurred at a frequency of 64 (49–98) /hour. When in automated control, a total of 18 manual adjustments were made in all 20 recordings (0.24 adjustments/hour), a reduction by 90% from the rate of manual adjustments observed during manual control (2.3/hour).”
From the above quote from the paper it is clear that automated control works to keep the saturation goal through roughly 7 X the number of adjustments than nursing makes per hour. It is hard to keep up with that pace when you have multiple assignments but that is what you need I suppose! The use of the auto setting here reduced the amount of nursing interventions to adjust FiO2 by 90% and yields tighter control of O2 saturations.
Dare to Dream
Self driving oxygen administration is coming and this proof of concept needs to be developed and soon into a commercial solution. The risk of O2 damage to developing tissues is too great not to bring this technology forward to the masses. As we prepare to move into a new institution I sincerely hope that this solution arrives in time but regardless I know our nurses and RRTs will do their best as they always do until such a device comes along. When it does imagine all of the time that could be devoted to other areas of care once you were able to move away from the non-invasive device!
Very interesting thoughts. Thanks for sharing.
What about the issue of oxygen cycling?