After several reports providing reassurance to breastfeeding mothers, two very recent reports are giving me reason to pause. The Canadian Pediatric Society has been recommending breastfeeding if a mother has COVID19 with precautions in place; Breastfeeding when mothers have suspected or proven COVID-19. It would be heresy to suggest that a mother not be permitted to breastfeed her infant but what follows are two reports that at the very least may need to enter the discussion when a COVID19 positive mother gives birth and is deciding about route of feeding.
Toronto Case Report
The first report was notable not so much for breastmilk but rather that a mother with a chronic immunodeficiency and pneumonia from COVID19 had placental surfaces that tested positive on PCR for COVID19. This was the main focus of the paper Probable congenital SARS-CoV-2 infection in a neonate born to a woman with active SARS-CoV-2 infection. In the same paper though, testing of breastmilk in this mother demonstrated a positive PCR with a semi-quantitative cycle time result (there are 40 cycles of amplification of RNA in PCR testing- the further away from 40 cycles the more likely it is a true positive).
The results above were positive at 2 days and negative at 7 days. One could possibly excuse this case as an anomaly since the mother in this case not only was sick but also has chronic neutropenia but then along comes another report.
Second Research Report
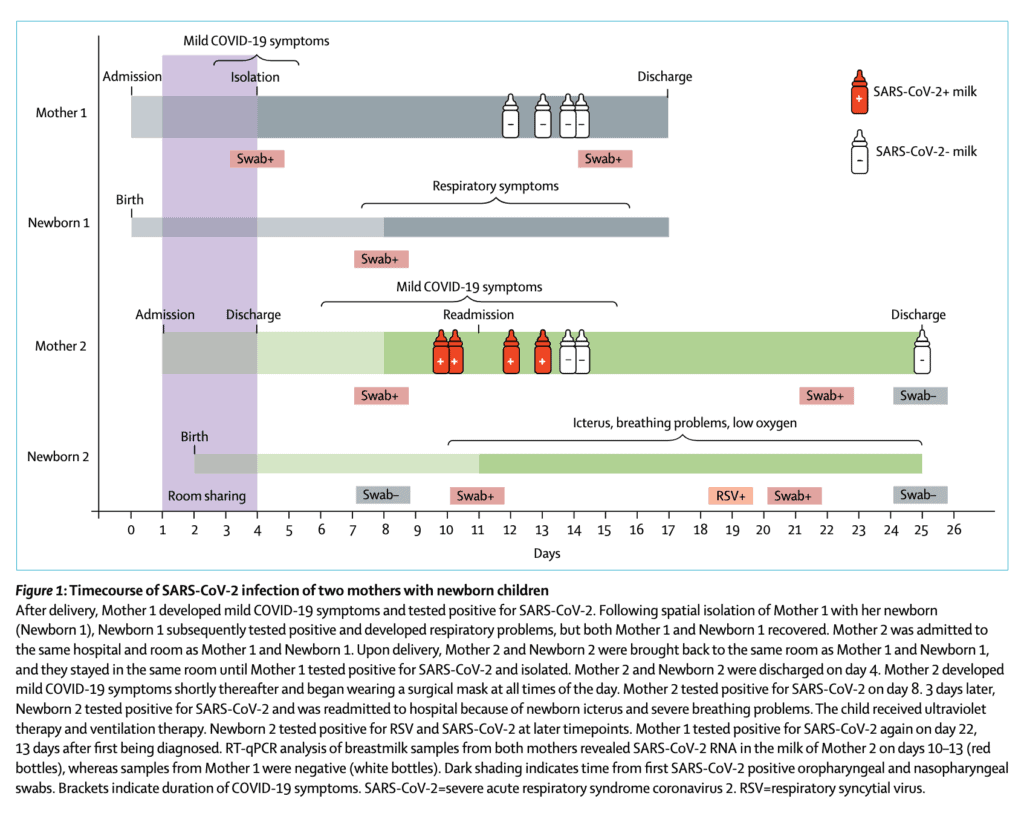
This week a second report emerged that adds to the uncertainty around breastmilk. Detection of SARS-CoV-2 in human breastmilk looks at two mothers one of whom was negative on testing of breastmilk but the other unfortunately tested positive. The authors included the following timeline which is very informative.
From the timeline above you will note that in the second case the mother becomes positive at 11 days of age and the infant tests positive around the same time the milk comes back positive. The infant in this case also develops RSV which likely explains the symptoms they developed later in the course. What is concerning to me though is that in this case while the mother was COVID19 positive, she was not acutely ill. When thinking of vertical transmission this has been something that has been postulated in suspecting that those with more severe illness have higher viral loads and therefore may be capable of vertical transmission. Not the case here if the results are to be believed. Adding to the strength of the result are Ct values for SARSCoV2 N peaked at 29∙8 and 30∙4 in whole milk and skimmed milk respectively so this seems real.
How does this differ than past testing?
What intrigues me about this study in particular is that past research on transmission into breastmilk has failed to detect the virus. It could be that previous testing close to delivery was negative and that with time might the virus enter breastmilk? At eleven days I think this may be the latest testing done. In virtually all cases reported about COVID19 positives in newborns the authors have always explained the painstaking steps they took to prevent postnatal infection. I do wonder now if some of these cases may be related to a small percentage of women carrying the virus in their breastmilk. This leaves us in a tough spot. What do we tell women who are thinking of breastfeeding and have COVID19? There will need to be discussion on this but one option is to proceed with feeding accepting there may be a small risk of transmission. A second option would be to test milk but if the transmission occurs late you may miss it in hospital on initial sampling Finally it may be worth pumping and discarding milk until mothers test negative and using donor breastmilk in the meantime (or formula for those who don’t have DBM).
Regardless I think this information coming out will need to be digested and centres think about how they will approach this issue. My guess is these will not be the last reports on this.
Breast milk is certainly a hot topic these days. Allergies in childhood are almost equally hot in the media as food allergies seem to be on the rise (not my specialty by a long shot) as well as rates of other atopic illness. Given what is known about the modifiable risks in terms of a number of conditions such as NEC and late onset sepsis in preterm infants it wouldn’t be a stretch to wonder what impact avoidance of cow’s milk exposure could have in the term newborn.
A Landmark Japanese Study
Urashima et al just published in JAMA Pediatrics the following paper Primary Prevention of Cow’s Milk Sensitization and Food Allergy by Avoiding Supplementation With Cow’s Milk Formula at Birth: A Randomized Clinical Trial . This paper looked at 312 infants (≥ 36 weeks at birth) who were randomized to either receive breastfeeding plus an elemental formula if needed vs breastfeeding plus intact protein cow’s milk formula with a volume of at least 5 mL/kg per day. In order to have a group of infants truly at risk of atopic disease, all infants had to have at least one immediate relative with atopic disease. In each arm of the study, infants were followed with blood IgE levels at 5 and 24 months of age to detect a level of CM-IgE ≥ allergen units/mL. This was the primary outcome on which the power calculation was based for the study. Using an estimated incidence of 10% in the breastmilk group vs 25% in the exposed group the authors needed 300 patients to detect a difference. Secondary outcomes included detection of other allergens aside from allergy to cow’s milk.
The Findings
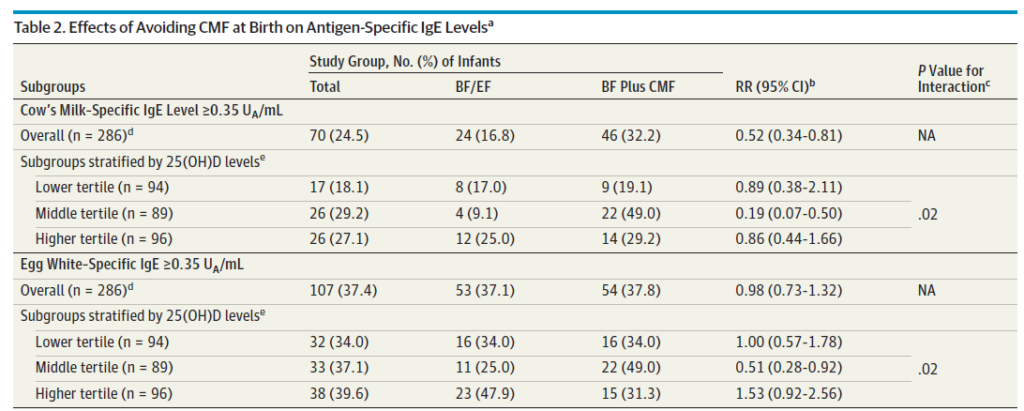
Given that I called this a landmark study it might not be surprising to know that they found a difference favoring protection with human milk.
Also curious is the relationship to vitamin D levels. Previous research has documented an inverse relationship between vitamin D levels in children and risk of atopy. Why only the middle tertile in this study but not the higher tertile had less IgE response is unknown.
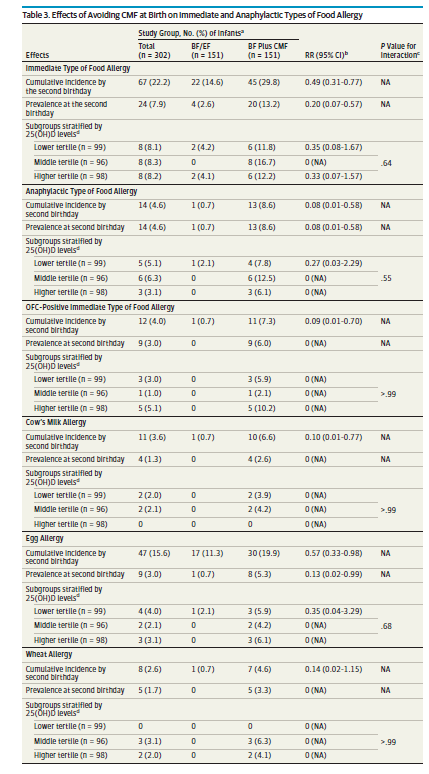
Perhaps even more surprising (at least to me) was that the risk of allergy at age 2 for other allergens was also lower.
Included in this lower risk was food allergy in general, risk of anaphylaxis and cow’s milk allergy that I presume manifested as rectal bleeding.
What Impact Could This Have
It is important to point out here that all these infants were ≥ 36 weeks so although I would love to infer that this strategy would have a huge impact on our preterm population I can’t say that yet (until a study is done). We certainly do see a fair bit of cow’s milk protein intolerance though that often leads to infants being placed NPO and on occasion worked up for NEC with a week or so of antibiotics. If this study is to be trusted, the rate of cow’s milk allergy was reduced from 6.6% to 0.7% in at risk infants (based on an immediate relative with atopy) and I would expect the risk in those without relatives to be less.
What might the impact be if we were to supplement with donor breast milk all term newborns who didn’t have enough maternal milk and take the elemental formula out of the equation entirely? If a 4 kg infant exclusively breastfed on day 1 and was give a couple ounces of supplement followed by full supplementation to 80 mL/kg/d on day 2 and then 100 mL/kg/d on day 3 that would total 26 ounces of donor milk in a worst case scenario assuming no maternal milk production during that time. At $4 per ounce we are looking at a cost to the system of about $100 a baby. Multiple that by the number of term infants in your centre to get an overall cost. In my own centre with about 12000 term deliveries a year that would come to 1.2 million dollars a year (again assuming no maternal milk at all). Is it worth the expense? I am not a health economist but I suspect if you were to add up the costs of workups/office visits etc for rectal bleeding, ED visits for asthma and anaphylaxis and the cost to families for food alleriges (let alone all the epi pens that need to be bought) it is worth it.
At the very least it does raise the question on post partum wards everywhere as to whether provision of cow’s milk formula should be one that someone has to consent to. With the publication of this study it certainly seems that it should be!
As a Neonatologist, there is no question that I am supportive of breast milk for preterm infants. When I first meet a family I ask the question “are you planning on breastfeeding” and know that other members of our team do the same. Before I get into the rest of this post, I realize that while breast milk may be optimal for these infants there are mother’s who can’t or won’t for a variety of reasons produce enough breast milk for their infants. Fortunately in Manitoba and many other places in the world breast milk banks have been developed to provide donor milk for supporting these families. Avoidance of formula in the early days to weeks of a ELBWs life carries benefits such as a reduction in NEC which is something we all want to see.
Mother’s own milk though is known to have additional benefits compared to donor milk which requires processing and in so doing removes some important qualities. Mother’s own milk contains more immunologic properties than donor including increased amounts of lactoferrin and contains bioactive cells. Growth on donor human milk is also reduced compared to mothers’ own milk and lastly since donor milk is obtained from mothers producing term milk there will be properties that differ from that of mothers producing fresh breast milk in the preterm period. I have no doubt there are many more detailed differences but for basic differences are these and form the basis for what is to come.
The Dose Response Effect of Mother’s Own Milk
Breast milk is a powerful thing. Previous studies on the impact of mother’s own milk (MOM) have shown that with every increment of 10 mL/kg/d of average intake, the risk of such outcomes as BPD and adverse developmental outcomes are decreased. In the case of BPD the effect is considerable with a 9.5% reduction in the odds of BPD for every 10% increase in MOM dose. With respect to developmental outcome ach 10 mL/kg/day increase in MOM was associated with a 0.35 increase in cognitive index score.
One of the best names for a study has to be the LOVE MOM study which enrolled 430 VLBW infants from 2008-2012. The results of this study Impact of early human milk on sepsis and health-care costs in very low birth weight infants.indicated that with incremental increases of 10 mL/kg of MOM reductions in sepsis of 19% were achieved and in addition overall costs were reduced.
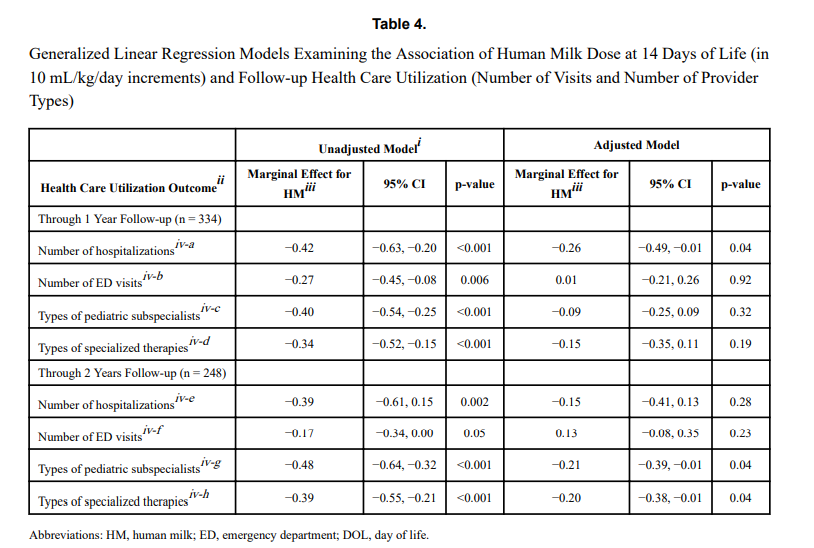
The same group just published another paper on this cohort looking at a different angle. NICU human milk dose and health care use after NICU discharge in very low birth weight infants. This study is as described and again looked at the impact of every 10 mL/kg increase in MOM at two time points; the first 14 and the first 28 days of life. Although the data for the LOVE MOM trial was collected prospectively it is important to recognize how the data for this study was procured. At the first visit after NICU discharge the caregiver was asked about hospitalizations, ED visits and specialized therapies and specialist appointments. These were all tracked at 4 and 8 months of corrected age were added to yield health care utilization in the first year, and the number of visits or provider types at 4, 8, and 20 months of corrected age provided health care utilization through 2 years.
What were the results?
“Each 10 mL/kg/day increase in HM in the first 14 days of life was associated with 0.26 fewer hospitalizations (p =
0.04) at 1 year and 0.21 fewer pediatric subspecialist types (p = 0.04) and 0.20 fewer specialized therapy types (p = 0.04) at 2 years.” The results at 28 days were not statistically significant. The authors reported both unadjusted and adjusted results controlling for many factors such as gestational age, completion of appointments and maternal education to name a few which may have influenced the results. The message therefore is that the more of MOM a VLBW is provided in the first 14 days of life, the better off they are in the first two years of life with respect to health care utilization.
That even makes some sense to me. The highest acuity typically for such infants is the first couple of weeks when they are dealing with RDS, PDA, higher oxygen requirements etc. Could the protective effects of MOM have the greatest bang for your buck during this time. By the time you reach 28 days is the effect less pronounced as you have selected out a different group of infants at that time point?
What is the weakness here though? The biggest risk I see in a study like this is recall bias. Many VLBW infants who leave the NICU have multiple issues requiring many different care providers and services. Some families might keep rigorous records of all appointments in a book while others might document some and not others. The big risk here in this study is that it is possible that some parents overstated the utilization rates and others under-reported. Not intentionally but if you have had 20 appointments in the first eight months could the number really by 18 or 22?
Another possibility is that infants receiving higher doses of MOM were healthier at the outset. Maternal stress may decrease milk production so might mothers who had healthier infants have been able to produce more milk? Are healthier infants in the first 14 days of life less likely to require more health care needs in the long term?
How do we use this information?
In spite of the caveats that I mentioned above there are multiple papers now showing the same thing. With each increment of 10 mL/kg of MOM benefits will be seen. It is not a binary effect meaning breastfed vs not. Rather much like the medications we use to treat a myriad of conditions there appears to be a dose response. It is not enough to ask the question “Are you intending to breastfeed?”. Rather it is incumbent on all of us to ask the follow-up question when a mother says yes; “How can we help you increase your production?” if that is what the family wants>
I woke up this morning and as I do everyday, scanned the media outlets for news that would be of interest to you the reader. One such article today was about how breast milk may give babies a metabolic boost due to micro RNA present in the milk. This got me thinking about how natural a thing this breast milk is and how substances within interact with the baby receiving it. After that point I recalled writing about a challenge to the statement that breast milk is natural and thought you might like to see what I considered to be an outrageous piece of journalism from last year.
The premise of the article is that by reinforcing that breastfeeding is natural we may hamper initiatives to increase vaccination in many parts of the world and in particular North America I would think. The idea here is that if we firmly entrench in women’s heads that natural is better then this will strengthen the conviction that we should not vaccinate with these “man made” unnatural vaccines. I am sorry to be dramatic about this but I think the argument is ridiculous and in fact dangerous.
The Definition of Natural
“existing in nature and not made or caused by people : coming from nature”
From the Mirriam Webster dictionary
Breastfeeding satisfies this definition pure and simple and there is nothing that anyone should say to suggest otherwise no matter what the motive is. The shift from formula to breastfeeding has been predicated on this notion and a plethora of literature on the subject demonstrating reductions in such things as infections of many kinds, diarrhoea, atopic disease in the first year of life as examples. In my world of premature infants additional reductions in NEC, bloody stools, have been seen and more recently in some cases improved neurodevelopmental outcomes.
In this case of irresponsible journalism a better approach if you were wanting to use the natural argument with respect to vaccines is to promote just that.
Vaccines are Natural
Someone will no doubt challenge me on this point as it would be a fair comment to say that there are artificial substances added to vaccines but there is no question the organisms that we vaccinate against are natural.
Think about this for a moment. All of the vaccines out there are meant to protect us against organisms that exists in NATURE. These are all bacteria or viruses that have likely existed on this planet of ours for millions of years. They are found everywhere and in many cases what we are doing when we give such vaccines are providing parts of or weakened versions of these natural organisms in order for us the human to mount a protective response.
This protective response is NATURAL. If we didn’t vaccinate and came across the fully virulent pathogen in NATURE our bodies would do exactly what they do when a vaccine is given to us. Our immune system would mount a response to the organism and start producing protective antibodies. Unfortunately in many cases this will be too little too late as the bacteria or virus will cause it’s damage before we have a chance to rid ourselves of this natural organism.
This is the basis of vaccination. Allow our bodies a chance to have protection against an organism that we haven’t been exposed to yet so that when it comes we have a legion of antibodies just waiting to attach this natural organism.
CNN Didn’t Get It Right
In the article which is based on a paper entitled the Unintended Consequences of Invoking the “Natural” in Breastfeeding Promotion by Jessica Martucci & Anne Barnhill the authors admit that the number of families that this actually would impact is small. the question then is why publish this at all. Steering families away from thinking that breastfeeding is natural is wrong. Plain and simple.
If the goal is to improve vaccination rates, focus on informing the public about how NATURAL vaccinations actually are and don’t drag breastfeeding down in order to achieve such goals. As a someone who writes themselves I am well aware of how personal biases creep into everything we write. I am aware of the irony of that statement since it is clear what side of the argument I sit on. While I peruse CNN myself almost daily I think the editors either missed the larger message in this piece or perhaps felt the same way. A disclosure that “the opinions of the author do not necessarily represent those of the network” does not cut it for what I would consider responsible journalism in this case.
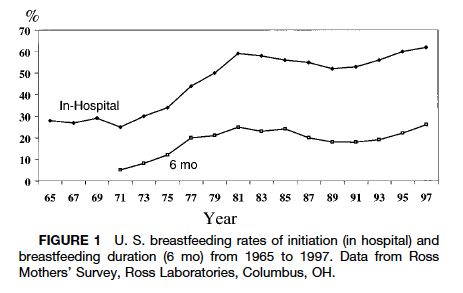
Nineteen seventy two was notable for many things aside from the year of my birth. Canada defeated the Soviets in the summer series, the Watergate scandal took down a Presidency, The GodFather was released and for the purposes of this post breastfeeding rates in the US reached an all time low of 22%. For an excellent review of the history of breastfeeding the article by AL Wright is excellent.
Rates of breastfeeding began a steady decline in the 1960s as more and more women entered the workforce and seemingly had to choose between employment and breastfeeding. This was a time when it was not seen as being acceptable to breastfeed in public (although that is not the case in many places still to this day) and the workplace was not as conducive to supporting women as in current times (think onsite daycares). Add to this that the 1970s also saw a backlash of sorts in the appeal of breastfeeding due to science “perfecting” a better source of nutrition in formula and we had the low rates that we did. In fact through discussions with parents from that generation, mother’s who chose to breastfeed may have been viewed by some as being silly for not using something like formula that could let the whole family in on the experience. Mom, Dad, kids and grandparents could all take part in the wonderful act of feeding. Why be so selfish?
Following this period as research began to demonstrate improved outcomes with breastfeeding including reductions in atopic disease, less hospital admissions and more recently positive impacts on intelligence and your microbiome the trend reversed. In fact, as the above graph demonstrates, rates approximating 70% were reached by the late 1990s. Since that time the CDC has shown that initiation rates have continued to rise and currently are at the highest documented levels in history.
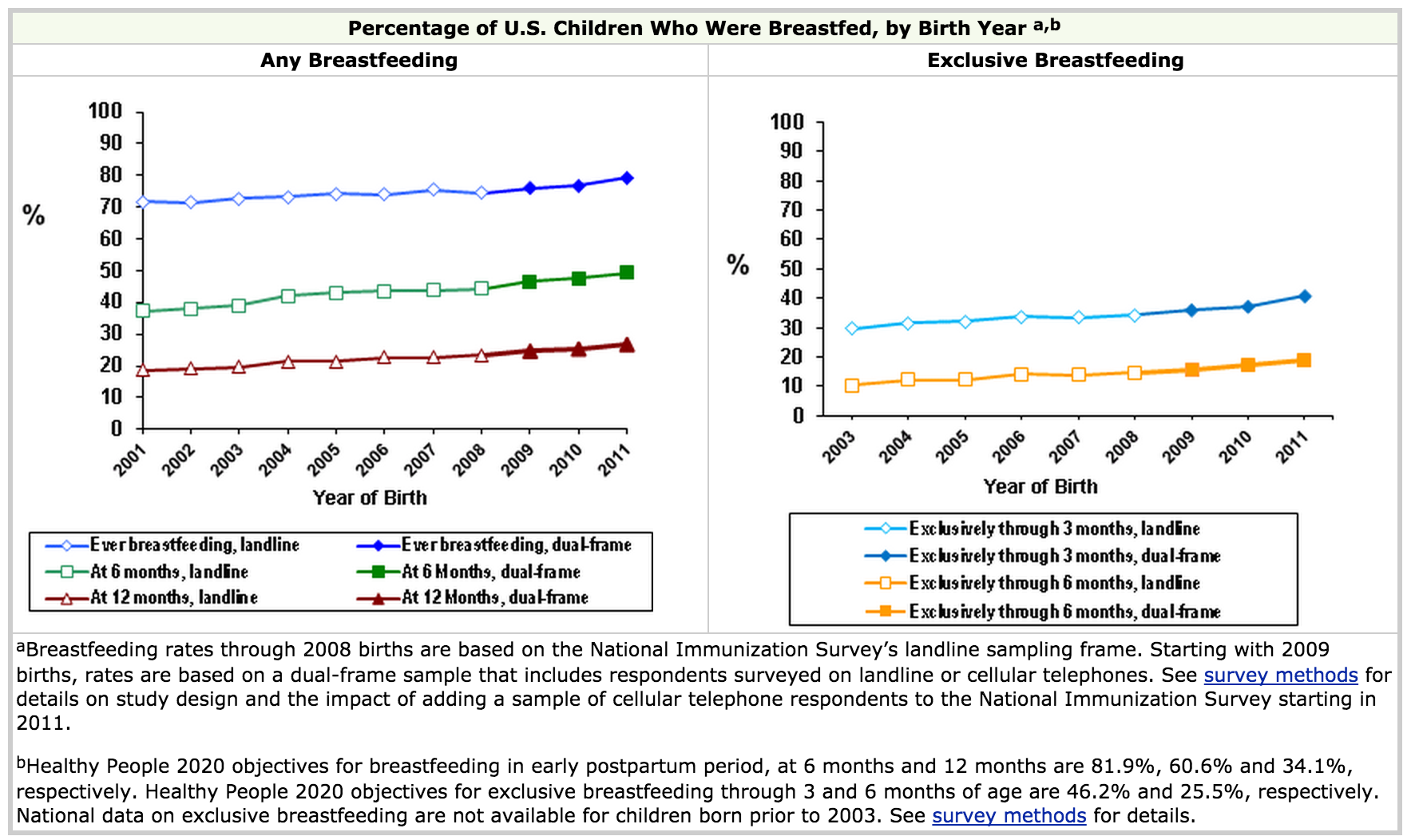
Looking at the CDC data though reveals some very important information. While the rates of any breastfeeding reach 80%, the rates at 6 months hover around 50%. This means that a significant portion of US women are using some formula when they come home and from the graph on the right about 35% by three months are exclusively breastfeeding. This number is far short of the goal the WHO has set to encourage exclusive breastfeeding for the first 6 months however it is a remarkable achievement for infant health.
http://www.who.int/topics/breastfeeding/en/
A recent trend on social media and print media has been the Brelfie. As you may know, this involves taking a picture of yourself breastfeeding your baby and posting it in one forum or another. This has been popularized by many celebrities and made it’s way onto the cover of Elle magazine this month.
So called Lactavists have been overjoyed to see such public acceptance and promotion of breastfeeding. As a Neonatologist I am delighted to see such high rates of breastfeeding and with it the beneficial effects that it brings.
Curiously, though all of this attention and promotion of breastfeeding has created a culture that is now being called bressure. This is defined as pressure to breastfeed and was the subject of a recent survey by Channel Mum in the UK. The highlights of the survey that went out to 2,075 mums showed:
– 16 per cent of bottle-feeding mums have been on the receiving end of cruel comments from other mothers they know
– one in 20 being attacked on social media
– 69 per cent of bottle-feeding mums said they had been judged negatively
– 41 per cent made to feel they have ‘failed as a mum and failed their child’ by not breastfeeding
– 15 per cent of mums have even lied to cover up their bottle-feeding and appear to be ‘better’ mums.
This so called bressure has led to a public campaign to increase awareness of the harassment that some mothers feel which involves taking selfies with cards having one word describing what breastfeeding meant for them. A video from Channel Mum can be seen here
While I am all for breastfeeding, I find it peculiar that the experience that breastfeeding mothers (all 22% of them) had in 1972 is now being felt by a larger percentage in 2015 who are bottle feeding. It is unfortunate that assumptions are being made of many of these women who put a bottle in the mouths of their infants. How many times does one conclude that the mother simply chose not to breastfeed because they were worried about the way their breasts would be affected cosmetically or that they simply chose to go back to work and breastfeeding would just get in the way. I suspect in most cases the truth is much different. Many of these mothers have tried to breastfeed but couldn’t produce enough. Others may have suffered from cracked nipples, mastitis, abscesses or due to prior surgery were unable to produce milk. Many such mothers have agonized over their “failure” to do something that they hear “everyone can do”. While they are told it takes some work for many that is a huge understatement. Is it not bad enough that these women have suffered the feeling of failure? To be looked at or spoken to in a disapproving way does nothing to support them. Add to this that by 3 months of age at least in the US 65% of mothers are providing some formula and it seems silly to take the “high and mighty” approach in the first couple of months and assume the worst of these women. Many of the “breastfeeders” will soon enough join the ranks of those using some formula.
Maybe the better option is to try and help. Many of the above problems whether it be producing enough quantity or pain related to breastfeeding can be addressed through tips on technique. While I am not an expert in this, hospitals would do well to increase staffing of on site lactation consultants to help mothers who wish to breastfeed get off on the right foot so to speak. A larger working force of midwives in North America in particular could certainly provide help in this regard. What I can say is that if a woman suffers a bad experience with breastfeeding in their first pregnancy the likelihood they will try again the next time is lower especially if we as a society make them feel like a failure.
Yes we need to promote breastfeeding and we should do what we can to follow the WHO recommendations and minimize the use of formula when possible. While bressure may have been intended to yield something good we need to be sensitive. Perhaps a better strategy next time a friend says they are going to use formula is to ask if they are having trouble with breastfeeding and if they need some help. Not having the discussion will ensure that nothing changes and a chance to do something will be lost due to misdirected bressure.
Its hard not to hear about probiotics these days. They are in our grocery stores as supplements to yoghurt and other foods and can be purchased in health food stores or at your local pharmacy. They appear to be everywhere as word spreads about the importance of your microbiome in maintaining good overall health.
It didn’t take long for clinician scientists to turn their attention to the neonate who is at risk of necrotizing enterocolits (NEC). It has been known for some time that formula feeding versus breast milk plays a role in the development of NEC as premature infants fed formula repeatedly were found across studies to have a higher incidence of NEC. The evidence is so strong in fact that the Cochrane review on the subject states “Enteral supplementation of probiotics prevents severe NEC and all cause mortality in preterm infants. Our updated review of available evidence strongly supports a change in practice.“ If you have read such reviews you know that they rarely come out this strong in their support of something! Furthermore, infants fed formula may have a different preponderance of more pathogenic bacteria in the colon and less lactobacillus and bifidobacterium species. The idea behind providing probiotics to neonates would therefore be to repopulate the intestine of these vulnerable infants with good bacteria and potentially reduce the incidence of a devastating condition like NEC.
If only it were that easy though
The issue of using Probiotics in preterm infants is a contentious one to say the least. While the evidence appears to indicate an overall benefit in terms of reducing rates of NEC there remain concerns regarding the safety of providing bacteria to this population even though the bacteria are thought to be beneficial. The people who urge caution in the use of probiotics say so due to a few reports of sepsis after the introduction of probiotics with the organism that the patient was provided or with a different species that was could be traced to a contaminated product. As noted in an article on CBC recently these products fall under the category of a nutritional product rather than a medication with Health Canada and therefore are not subject to the same rigorous quality control standards as other comparable medications would be.
Others while recognizing the potential for contamination and sepsis would argue that the risk is low compared to the benefit provided to the infants overall and therefore claim benefits outweigh risks.
Manipulating Breastmilk in a Double Bling RCT
Given the above concerns regarding administration of these products to neonates I was excited to see the randomized double blinded study by Benor S et al; Probiotic supplementation in mothers of very low birth weight infants. This study enrolled mother and infant pairs within 72 hours after birth to commence on maternal treatment with Lactobacillus acidodphilus and Bifidobatera lactis versus placebo until discharge. The rationale for giving probiotics to lactating mothers was based on a previous study showing less atopic dermatitis in the offspring of mothers who took such treatment while breastfeeding and in a study of breast milk demonstrating lower levels of the inflammatory cytokine transforming growth factor beta (TNF-B). Less inflammation might equate to less NEC.
The primary outcome was Bell Stage II NEC and the investigators required 90 mothers in each arm to show a difference in the incidence of NEC based on previous work in their centre. All included pairs needed to be providing >50% EBM in order to minimize any effect from formula. The overall incidence of NEC at the completion of the study was 27% in the placebo group vs 12% probiotic group and for NEC II 18% vs 4% in those treated with probiotics. The rates of NEC were quite high compared to what we typically see and the authors noted that even for their site (for uncertain reasons) there was a higher rate than they expected. Neither of the rates of NEC were statistically different (both reached p=0.15 levels) but there was a significant issue with this study.
The total recruitment was 25 in the probiotic and 33 in the control arm. This was a far cry from the estimated 90 needed per side. The reason for this goes back to the start of this blog entry. The study needed to be stopped due to poor enrolment. Why so low? The majority of mothers approached for this study did not want to risk not getting probiotics so they opted to simply take them due to the perceived health benefits that as adults they already believe exist. Sadly I think this problem would resurface in many places if the study was replicated. This loss of equipoise by the families will make obtaining consent for such studies very difficult and we may not get a satisfactory answer.
Interestingly the authors of this study also measured TNF-B and found a strong trend towards lower levels in the breast milk of the probiotic supplemented group matching the trend towards less NEC.
I sincerely hope that another study such as this can be done without such issues in recruitment as the strategy would address the issue of not providing the bacteria directly to the neonate while still potentially reaping the benefits of less NEC. For now we will have to wait and see.







 So called Lactavists have been overjoyed to see such public acceptance and promotion of breastfeeding. As a Neonatologist I am delighted to see such high rates of breastfeeding and with it the beneficial effects that it brings.
So called Lactavists have been overjoyed to see such public acceptance and promotion of breastfeeding. As a Neonatologist I am delighted to see such high rates of breastfeeding and with it the beneficial effects that it brings.