I will admit it. I resist change at times just like many others. This may come as a surprise to some of you who have worked with me and accused me of bringing too much change at times to the units. The truth though is that when one understands something and is enthusiastic about implementation the change does not seem so difficult. When it isn’t your idea though we may find ourselves a little uneasy about adopting this unfamiliar practice.
Such has been my experience with nasal HFOV. It is a strategy that has been around for over five years but has seen slow adoption among centres in Canada and has trickled into practice in Winnipeg on a few occasions. In each occasion when I have been asked about either continuing or perhaps starting this therapy I have shrugged my shoulders and confessed my inexperience with the modality. Sure I have used HFOV through an ETT but through prongs or a mask?! How would it work? Could it cause harm? What would the actual indications be? How would our in house physicians and NNPs respond to abnormal gases overnight even if I felt comfortable with using it? These sorts of questions have led to virtual inertia in my acceptance of the strategy.
Before I go on it would be good to see an example of how it is set up. The MedinCNO device is capable of delivering such non-invasive HFOV and can be seen in this short video.
One could use the strategy either prophylactically to extubate an infant or as rescue to prevent reintubation if trials of either CPAP or NIPPV were unsuccessful. HFOV is known to be very effective at clearing CO2 when used through an ETT so perhaps nasal application could also lower pCO2 and achieve a similar effect. This was tested using a neonatal lung simulator by Mukeji A et al Nasal high-frequency oscillation for lung carbon dioxide clearance in the newborn. In this study CO2 was introduced into the manequin and the amount of exhaled CO2 determined while on CPAP, NIPPV and nasal HFOV. Interestingly during CPAP no exhaled CO2 could be detected while CO2 clearance occurred during NIPPV and nasal HFOV although it was three-fold greater with HFOV. In theory then CO2 clearance would appear to be better so in the case of ventilatory failure as evidenced by CO2 retention this modality would seem to win out.
Clinical Evidence for Use
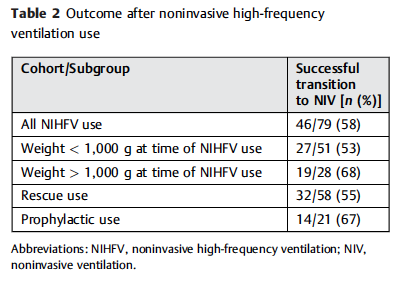
There is one RCT in term infants with TTN to support the practice while the rest are unblinded case series with no controls. Four Canadian NICUs recently described their experience however using a retrospective analysis. Included were 79 instances of HFOV distributed as follows; 73% utilized as rescue from another mode and in 27% used as the primary mode for extubation. The outcomes are shown in the table:
In 45% of cases the patients needed intubation after first trialing CPAP or NIPPV while in 33% of cases following extubation the infants needed replacement of the endotracheal tube. The numbers here are small so it is difficult to truly compare them to other studies with confidence but reintubation rates of 40-44% have been noted recently when using NIPPV or CPAP so the numbers are at least consistent.
One aspect though that caught my eye was the duration of use for HFOV across these 79 patients. The median use was 57 hours with the longest duration being just over 400 hours. It would seem that the use of this modality for the most part is as a bridge to something else. The median duration of 2.5 days is much shorter than the weeks that some of our smallest infants remain on CPAP/NIPPV for. Whether for rescue or prophylaxis this is not a long term option.
Another point worth noting though is the question of whether it is the pressure or oscillatory wave that is leading to success. As the authors note, there were a wide range in applications of MAP, delta P and frequency.
MAP ranges from 8 – 24 cm H2O while frequency from 6 – 14 hz and amplitude varied widely depending on the device used but was as high as 100%. While high MAP has been used invasively though an ETT I can’t help but wonder if in some cases the real benefit was the high MAP. What would happen for example if the centres had simply raised the CPAP to 10, 12 or even higher?
In the end it would seem that in principal it is an effective therapy that may be able to remove CO2 more efficiently than the other modes. What we don’t have are RCTs in the smallest babies comparing HFOV to NIPPV or CPAP with adequate power to detect differences. I suspect these will come soon enough but what do we do in the meantime? The main reservation I have has to do with safety. We truly have little if any data on this without proper trials to ease such worry. When a patient is in front of us though and is failing CPAP or NIPPV what are we to do? Should we intubate or trial this modality based on the evidence thus far?
I might be tempted to trial HFOV in this circumstance but as with any new therapy we need education for all staff. Everyone caring for our infants need to understand what they are using and how to respond based on clinical findings. This is the real issue with safety that I see and until such time that we have widespread education across RRT, nursing and medicine I would suggest we use this with trepidation. This is not a rejection of the modality in the least but rather a call to come together as a team and see how implement this in such a way that will provide direction to caregivers, provide a consistent approach with respect to length of use, indications and when to change direction entirely. Time to call a meeting of the minds I think.
Another year has passed and another World Prematurity Day is upon us. I thought about what to write for this day that draws attention to premature infants worldwide and was hit with many ideas which no doubt will form the basis for many posts to come. There was one thought that struck me though as being so important to think about as we push forward, striving to improve survival across the globe for our smallest patients. There is no doubt that you will have heard the expression “just because we can do something, should we?” In 2015 I don’t think this applies more than at this very moment.
At a Tipping Point
You see we are at a tipping point as Malcolm Gladwell explained so brilliantly in his book by the same name. In April of 2015 Rysavy et al published the results of survival and morbidity data for infants born in 24 US hospitals between the ages of 22 – 26 weeks. The nearly 5000 infants included demonstrated two very important things. Firstly, survival is possible at 22 and 23 weeks and there is a chance, albeit less than 50% that these infants will survive without moderate or severe disability. Secondly, at these gestational ages 75% of hospitals included provided active resuscitation to these infants. Given that this is the largest study out there and shows that survival is possible and we can expect to see some good outcomes it would seem logical to move forward with universal resuscitation of these infants would it not?
You Are Going To Practice on What?!
As the saying goes though, “Perfect Practice Makes Perfect”. Not all hospitals have equal performance at these gestational ages which is demonstrated in the ranges of outcomes across hospitals as shown in the Rysavy paper. To even suggest that we need to practice on premature babies will no doubt leave many of you feeling queasy but in essence that is what is truly needed to improve our outcomes further. An infant born at 22 – 24 weeks is vastly different than one born at a later gestational age. Their skin is extremely fragile and prone to breakage with resultant risk of infection. Their lungs are in a stage of development that has yet to produce any real abundance of gas exchanging alveoli and their brains lacking the sulci and gyri that are to come many weeks later. They are in need of meticulous “best practice” care and without that their outcomes are certainly to be influenced. Depending on the centre though, you may see 5, 10, 15, 20 patients a year at these ages. How can a team possibly gain enough experience in treating these children appropriately if they see 1 or 2 every two months? Add to this that you may have 10 different Neonatologists so on average each of you may take care of one patient a year at birth. This is a recipe prone to poor outcomes if you ask me.
The Evolution of the Small Baby Unit
The answer no doubt will lie in creating smaller teams; so called “Small Baby Units”. Such units have small groups of health care providers dedicated to treating such infants thereby increasing the frequency of individuals exposure to these babies. There is some recent evidence published in Pediatrics that supports this notion. Small Baby Unit Improves Quality and Outcomes in Extremely Low Birth Weight Infants. In this study a period of two years before and four years after opening such a unit were compared across a number of measures. The findings were as follows “There was a reduction in chronic lung disease from 47.5% to 35.4% (P = .097). The rate of hospital-acquired infection decreased from 39.3% to 19.4% (P < .001). Infants being discharged with growth restriction (combined weight and head circumference <10th percentile) decreased from 62.3% to 37.3% (P = .001). Reduced resource utilization was demonstrated as the mean number per patient of laboratory tests decreased from 224 to 82 (P < .001) and radiographs decreased from 45 to 22 (P < .001).” I hope you would agree that achievements such as these are worth the effort to create such an environment. Future studies I believe will confirm these findings although having the gold standard RCT may be difficult to achieve as I suspect we will have lost equipoise.
This brings me to the final point though and that is whether we are ready as a health care system for the increase patient load that this change will bring about. Based on an expected stay of 4 months for a baby born at this age and knowing the average number of such babies delivered per year, we would be looking at about 600 patient days per year added to each hospital’s occupancy in our two centres. This represents about a 5% increase in patient bed days per year. Five percent may not seem like a large increase at first blush but when we like many hospitals have been trying to deal with staffing issues and many days in which we are at or near capacity, this is not an insignificant challenge. It is a challenge though that we must face head on. Resources must be found, and space provided to accommodate for these children. We live in a world now where it is not solely up to us but to the family as well who must be integral to any such decision to either pursue or withdraw care. News of such infants surviving has spread to the public and I have no doubt that many families will have heard stories of such survivors. The next phase of care for these infants must address the shortcomings in care at the moment.
How do we educate families about what to expect in the long run?
How do we support these families when they make such difficult decisions either way?
How do we support our front line staff who may hold quite discrepant viewpoints about what is “right” yet expect them to function as one team moving clearly in a direction that supports the family?
How do we ensure that our focus on our smallest infants does not distract us from the attention needed by those born at later gestational ages?
I could go on but these are just some of the questions that I hope the next year begins to tackle. We are in the midst of an evolutionary point in Neonatology and we owe it to ourselves and the families we care for to navigate this change as best we can.
Something kind of big happened today. I received a notice on my Facebook Page that there were now 3000 “likes” for this little community that I started back in February of this year. I was asked early on what the purpose of this blog and Facebook page were and in response I wrote the piece Inside the mind of a Neonatal Blogger. Why am I doing this?. If you are curious, this gives you a good glimpse into my motivations.
Truth be told though I wasn’t really sure what this would become and early on my goal was to have 300 likes and then when that was passed 1000. What has happened since has been quite the surprise. I could not have imagined the growth in the page and the blog since that time.
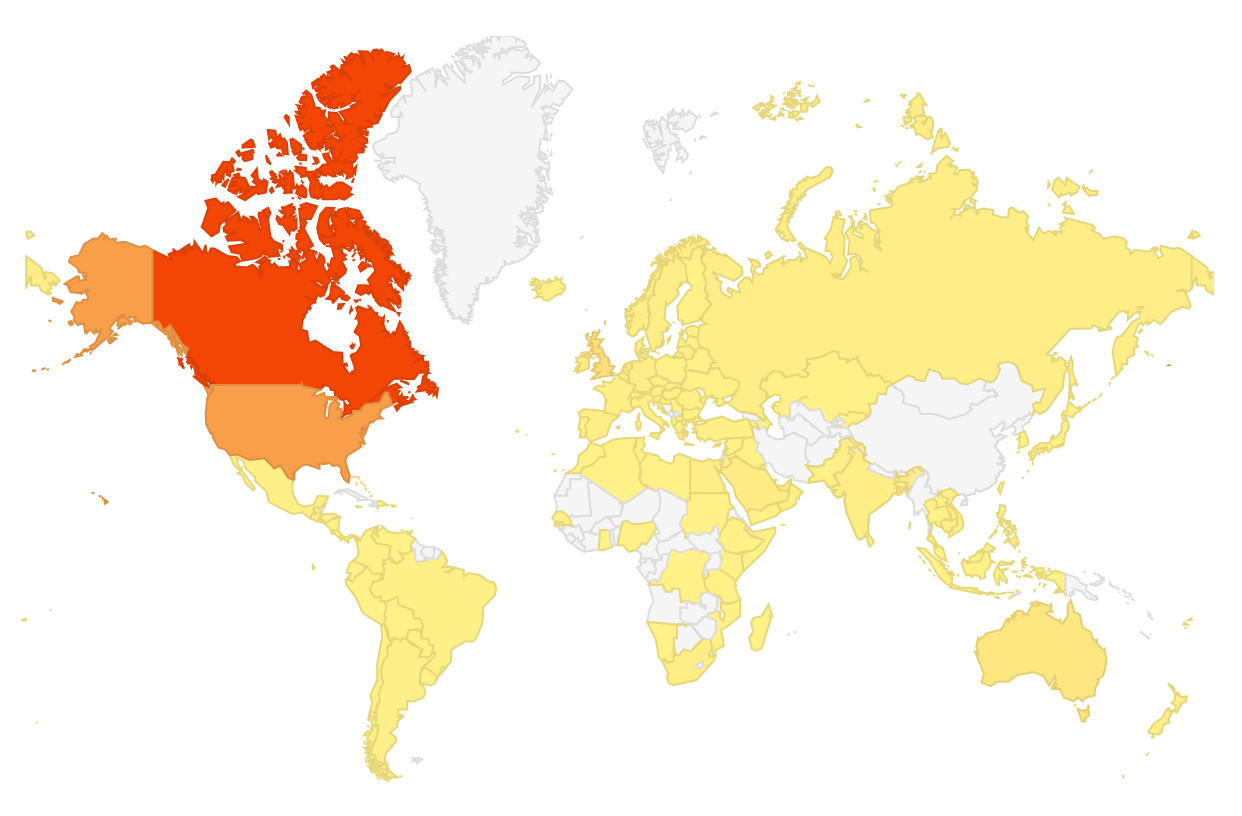
The map above actually represents all the countries that have read posts from this blog. The red colour aside from being Canada indicates the top country in terms of views, the USA is second in orange and then yellow being the rest of the countries on the map. The white areas are as of yet countries that have not read a piece but who knows what will happen given a little more time!
An interesting shift though has occurred on the Facebook page and that is over the last month a real community has evolved. Up until recently a given post might generate one or two comments but I have noticed something quite special evolving on this site. That is that not only have the comments increased with each post but you the readers are beginning to use this site as I had envisioned. Comments are being made and you are responding rather than leaving it all up to me. Don’t take this the wrong way though, I am more than happy to respond but I am enjoying reading your own thoughts as well. We come from such a wide variety of backgrounds and experiences and these differences are beginning to express themselves in your written words.
As much as I enjoy finding interesting Neonatal content to share with you, I equally enjoy seeing how you respond. An additional complement is that the interactions are almost always respectful, productive and generating of even more dialogue. I learn from you just as you learn from me so let me say thank you for that!
Lastly, I have come to understand that “All Things Neonatal” really does have to be just that. Try as I might I have not been able to unlock the secret of what truly interests the reader. Topics that I would have predicted would “go viral” have been put out into the internet only to produce a sound “thud” as they fall flat which others that I might have thought would generate mild interest have exploded. It is this unpredictability that keeps me excited about putting out each post as I continue to be fascinated by my inability to predict what leads to a boom or a bust.
In case you are wondering though the top three posts have been:
If you haven’t read these then you may be missing out as your fellow readers seemed to think these were a big hit.
Thanks to each of you for following and keep the comments coming. Also if you try something out that you see on this site and adopt it in your hospital please let me know how it has gone. We can all learn plenty from each other. As our base grows so does our collective knowledge and in my opinion that is a good thing.
The 10th Annual Bowman Symposium did not disappoint! World class presenters gathered to provide a top to bottom update on a variety of topics spanning from the nervous system to Genetics. After a day and a half of presentations though I was left with some concerning (scary) thoughts and it seemed Halloween was the perfect time to share them with you!
How Much Oxygen is Just Right?
Dr. Ola Saugstad provided a wonderful history of the use of oxygen in Neonatology. After his talk it was clear that oxygen is most definitely a drug with its most concerning side effect being the production of oxygen free radicals in the body. If we are too restrictive aiming for saturations of 85 – 89% we spare our infants ROP but put them at greater risk of death. Too high at 91 – 95% and they may survive but with more ROP (BOOST and SUPPORT). If we resuscitate with 100% oxygen that is associated with worse outcomes but so too is 21% in our newborns < 28 weeks. The NRP would advise us to use 21 – 30% to start in this group for resuscitating but he recommends 30%. Certainly the recent publication by Jack Rabi out of Calgary suggests room air may in fact be harmful in this group as a starting point! After 50 years of research we still don’t know what to give newborns to help them start their life outside the womb. Scary.
It’s All In The Name
Next up is Dr. Aviva Goldberg who raised a very important point that I had not considered before. In every researchers quest to come up with a catchy name for their study that people will remember, the connotation is equally important. The SUPPORT study came under heavy fire (commentary here) after a surprising increase in mortality was found in the arm randomized to 85 – 89% saturations. Families sued the investigators and in their complaints they were angry about being misled. How could a study that was named the SUPPORT study do anything other than help their children? The title in and of itself they argued misled them as they never would have thought increased mortality could be a risk. Researchers make sure you test out your clever names with parents before finalizing your studies. The decision otherwise could come back to haunt you…
Jury Still Out on Bevicizumab (Avastin) for ROP
Dr. Ian Clark provided an overvue of the current state of thinking on treating ROP. For central disease in Zone 1 Avastin is preferred but for more peripheral disease laser seems to still be recommended due to its decisiveness in eliminating the disease without affecting future vision. Concerns continue though with respect to potential systemic effects of putting an anti-VEGF medication in the eye. Can it leak out and cause disruption to angiogenesis in other organs and in particular the brain? A recent poster at the CPS meeting in Toronto entitled Neurodevelopmental outcomes of extremely preterm infants treated with bevacizumab for severe retinopathy of prematurity indicates that there may be greater impairment in those receiving injections. There are several flaws in this paper though including greater numbers of males (we always do worse), more sepsis and worse SNAP-II scores in the injection group but the results have been making it into discussions leaving Ophthalmologists wondering if they are doing the right thing…very scary.
Cow’s Milk Human Milk Fortifier Is Safe For Premature Infants… Or is it?
Next up was Dr. Bill Diehl Jones who presented in vitro data on the effect of these supplements with respect to their contribution to oxidative stress. Such stress has been associated with BPD, NEC and ROP to name a few disorders in preemies. A paper published this week in which intestinal cells were exposed to human milk with HMF experienced significantly increased intracellular oxidation, cell damage, and cell death compared to those exposed to just breast milk. A paper from 2013 indicates that premature infants fed HMF experience increasing levels of urinary isoprostanes (a measure of oxidative stress). We know that infants receiving these products experience better growth and bone density than those without exposure but is there a cost? Will further research in this area drive us towards exclusive human milk based diets? The seed that has been planted in my head now questioning the safety of this product I use every day…a little frightening.
Curtailing Antibiotic Use And The Coming Black Swan
John Baier spoke about practice variation between Neonatologists in terms of the decision to prolong antibiotics or not in the face of negative cultures. While we do have variation, the good news is that we overall have cut down our tendency to prolong past 48 hours in the face of negative cultures. If we practice long enough though, the Black Swan will eventually rear its ugly head. The Black Swan is an exceptionally unusual event but one that has dramatic impact. How will we respond when a patient becomes septic after 48 hours and the antibiotics were stopped? Will we panic and change our practice entirely to avoid the internal pain again of feeling like we made a mistake or remember that we have saved countless infants from the long-term effects of indiscriminate use such as NEC, atopic disease and obesity in childhood just to name a few. It is this nagging doubt I have about how we will react that gives me cause to worry!
Finishing With a Miracle
It doesn’t seem right to end on a down note so I thought it would be worth celebrating that a cure has been found for something very scary. Hypophosphatasia is a rare disorder of the bone which was previously lethal in many cases. Thanks to research that our own Dr. Cheryl Greenberg led here in Canada we are able to successfully treat these children now. The Bowman symposium showed us incredible videos of such treated children and to end this post I found this video from Youtube of Gideon who was one of these patients treated with FDA Okays Asfotase Alfa (Strensiq). If you would like to leave this post with a smile on your face until next Halloween have a look at the video!
Elon Musk, a name synonymous with technology in our time (as the brains behind the all-electric Tesla automobile), had this to say about the “Good Old Days”
“If anyone thinks they’d rather be in a different part of history, they’re probably not a very good student of history. Life sucked in the old days. People knew very little, and you were likely to die at a young age of some horrible disease…”
I wonder what he would say though about Sister J Ward who worked in the premature unit at Rochford General Hospital, Essex in the 1950s. It was during this time that she took a baby outside with her to enjoy a warm afternoon. Upon returning to the unit and taking off the sheet that accompanied the child she noticed a discrepancy between the yellow colour which remained under the covered skin and that which had been exposed to sunlight. Her observation led her to conclude that the sunlight had in fact been responsible for the change (and she was right!) but her conclusion was largely ignored.
Soon thereafter a tube of blood provided the convincing evidence that the sun was in fact directly responsible for such a change. This tube which had been left on the windowsill in the sun was tested for a bilirubin level and found to be low. As the care providers felt the test was inaccurate a repeat sample was drawn and the fresh tube contained a much higher level. A repeat sample of the blood that was again left in the sun showed an even lower level than previously seen inspiring researchers to seek out the effect of light on bilirubin. This ushered in the age of phototherapy lamps that are used around the world today. The design of such lamps has undergone many changes with the current models mostly focusing on the generation of light in the blue spectrum. Mostly gone in the developed world are the long phototherapy bright light tubes that were ubiquitous when I was in residency. It didn’t start off that way though. All you needed was a little golden sun!
A Randomized Trial of Sunlight to….
This month in the New England Journal of Medicine a non-inferiority study has been published comparing conventional phototherapy with BiliBlankets to you guessed it…sunlight. The study took place in Nigeria where such a study is both practical and possible. Conducting the study in Winnipeg for example would yield a treatment that could be used for 3-4 months a year at best but in a more temperate part of the world it indeed is a reasonable question to ask. The infants randomized to sunlight were placed under filtered light using either a canopy made of an Air Blue 80 film on overcast days or when sunny, in a Gila Titanium film. These films have been shown to essentially block all UV light while allowing light in the blue spectrum through. Aside from Sister Ward demonstrating that sunlight was an effective treatment for jaundice over 60 years ago, a significant motivation for determining if sunlight could be employed is the cost difference of the two strategies. A BiliBlanket will cost between 2-3000 dollars each while these canopies can be made for $0.55 and $1.50 per square foot of film type respectively and $44 and $120 for a canopy for six to eight mother–infant pairs with Titanium and Air Blue 80 films. In countries where resources are scarce one can see the compelling reason to try such a strategy.
The Results
The criteria for efficacy were twofold. The first outcome was achieving a rate of increase in total serum bilirubin of less than 0.2 mg per deciliter per hour for infants up to 72 hours of age or secondly a decrease in total serum bilirubin for infants older than 72 hours of age who were receiving at least 5 hours of phototherapy. After comparing 250 courses using sunlight to 311, five hour exposures to BiliBlankets, sunlight was found to be equally effective. Interestingly, the spectral irradiance (measure of the intensity of the light source) however was significantly higher in the group receiving sunlight 40 vs. 17 μW per square centimeter per nanometer, P<0.001. Additionally, the total area covered was greater under the canopy which may help to explain why in a secondary analysis the rate of decline in bilirubin was found to be faster with sunlight.
But is it safe?
Putting babies under the sun for 5 hours would seem to go against everything we have been taught but remember this was filtered light so sunburn was not a concern. Temperatures were monitored for all children and if necessary they were moved into the shade to cool off or in other cases on quite hot days prophylactic cool towels were applied intermittently. In the end though only one baby recorded a short-lived temperature over 39 degrees, no babies became dehydrated and in only one case was a doctor called to see a child.
Final Thoughts
We are blessed to live in a country where we have ready access to phototherapy blankets, overhead lights that are either independent free units or integrated into expensive neonatal beds. This is not always the case in the developing world. I find it simply amazing that a discovery over 50 years ago that led to the development of an entire industry would one day be simplified back to where it all began. We must not forget that while bilirubin encephalopathy leading to kernicterus is rare in the developed world, in places without access to phototherapy it is a real and present danger. We now know that the most naturopathic treatment of all; the sun which is free and readily available is just as effective and possibly more than our high-tech devices.
Elon Musk may be one of the most brilliant inventors of the modern era but with respect to caring for babies with yellowing of the skin, Sister Ward had a leg up on him.
On occasion two articles will be published in short succession and have discrepant findings. This appears to be one of those times. Hishikawa K in Japan published a paper in September entitled Pulmonary air leak associated with CPAP at term birth resuscitation while Calebi MY from Turkey published Impact of Prophylactic Continuous Positive Airway Pressure on Transient Tachypnea of the Newborn and Neonatal Intensive Care Admission in Newborns Delivered by Elective Cesarean Section in August of this year.
The findings as we will discuss were quite discrepant which on the surface leaves the practitioner in a quandry. How do I best treat my patients? The key difference between the two studies was the finding of an increased rate of pneumothorax in the study by Hishikawa when CPAP was used in term infants with respiratory distress after delivery. Curiously prophylactic CPAP of +5 was used in both studies but the populations under study were quite different. The study by Calebi targeted infants between 34 0/7 weeks and 38/6/7 weeks vs term infants in the study from the Japanese group.
Another important difference is the utilization of CPAP which in the study by Calebi involved prophylactic administration within twenty minutes of birth and in the Japanese cohort the indication was the development of symptoms. Thinking about this for a moment, these two groups are actually quite different. A newborn with TTN has an increased amount of interstitial fluid that has not made it’s way to the hilum for reabsorption in the lymphatic system. The lungs of these infants are heavier with fluid than comparable infants without such pathology and therefore are also less compliant. Non compliant lungs are prone to microatelectasis as the infants progressively experience alveolar collapse. The longer the clinician waits to start supportive CPAP the more the lungs collapse and greater negative pressure is required to open these closing alveoli. Furthermore if there is fluid in the airway itself there is the potential for a ball valve mechanism to come into effect whereby air is able to pass through the dilated airways during inspiration but on expiration the collapse leads to air trapping. Such trapping places the infant at risk for air leak. CPAP is used to establish an adequate functional residual capacity (FRC) as indicated in this picture. Failure to do so results in atelectasis.
The Japanese study examines the impact of CPAP after a change in guidelines in 2010 suggesting that CPAP should be utilized in the delivery suite for those infants with ongoing respiratory distress. The study by Calebi really examines a different patient group being those who are near term patients with TTN who have early CPAP implemented. The early administration of CPAP may be the technique that prevents alveolar collapse as mentioned above and avoids the requirement by the infant to generate such high negative pressure with its inherent risk of air leak.
Is All CPAP The Same?
Another important distinction between the two papers is the way in which CPAP was administered. The Japanese utilized a flow inflating bag with a pressure valve and manometer while the study by Calebi employed a T-piece resuscitator. When it comes to maintaining CPAP there is no question having used both devices that I find the T-piece resuscitator much easier to use and over longer periods the reliability of the pressure delivered by the T-piece would be superior to that with the flow inflating bag. The Neopuff T-Piece Resuscitator possesses a pressure relief valve which could help during an instance when the patient is crying or breath holding. The constant flow without a relief valve could lead to airleak which is precisely the situation that may occur during the use of a flow inflating bag.
Yes there was over a three fold increase in airleak at near term gestational age in the Japanese cohort but this was not seen at all in the Turkish study in which CPAP was implemented early. So the message here is that if you start CPAP early enough you can prevent airleaks from occurring. This in and of itself is worth implementing.
Can CPAP Reduce Hospital Admission to NICU?
There is more to the story however. The Turkish group demonstrated a significant difference in admission rates to the NICU as shown in the following figure. The results here although just achieving significance should not be minimized. Avoiding progressive atelectasis decreases admission rates. The conclusion here is that there is little benefit in adopting a wait and see approach to those kids born by elective c-section. While it is true that you may be treating a significant number of healthy patients between 34 0/7 – 38 6/7 weeks with CPAP it is for a brief period and makes a significant difference in frequency of admission.
We live in an era of bed shortages and I would argue that anything we can do to reduce admissions and moreover keep babies with their parents is worth exploring. From my perspective treating these kids with the appropriate CPAP device for twenty minutes after birth is well worth it. Perhaps your unit should consider the same.



 In April of 2015
In April of 2015  This represents about a 5% increase in patient bed days per year. Five percent may not seem like a large increase at first blush but when we like many hospitals have been trying to deal with staffing issues and many days in which we are at or near capacity, this is not an insignificant challenge. It is a challenge though that we must face head on. Resources must be found, and space provided to accommodate for these children. We live in a world now where it is not solely up to us but to the family as well who must be integral to any such decision to either pursue or withdraw care. News of such infants surviving has spread to the public and I have no doubt that many families will have heard stories of such survivors. The next phase of care for these infants must address the shortcomings in care at the moment.
This represents about a 5% increase in patient bed days per year. Five percent may not seem like a large increase at first blush but when we like many hospitals have been trying to deal with staffing issues and many days in which we are at or near capacity, this is not an insignificant challenge. It is a challenge though that we must face head on. Resources must be found, and space provided to accommodate for these children. We live in a world now where it is not solely up to us but to the family as well who must be integral to any such decision to either pursue or withdraw care. News of such infants surviving has spread to the public and I have no doubt that many families will have heard stories of such survivors. The next phase of care for these infants must address the shortcomings in care at the moment.



 It was during this time that she took a baby outside with her to enjoy a warm afternoon. Upon returning to the unit and taking off the sheet that accompanied the child she noticed a discrepancy between the yellow colour which remained under the covered skin and that which had been exposed to sunlight. Her observation led her to conclude that the sunlight had in fact been responsible for the change (and she was right!) but her conclusion was largely ignored.
It was during this time that she took a baby outside with her to enjoy a warm afternoon. Upon returning to the unit and taking off the sheet that accompanied the child she noticed a discrepancy between the yellow colour which remained under the covered skin and that which had been exposed to sunlight. Her observation led her to conclude that the sunlight had in fact been responsible for the change (and she was right!) but her conclusion was largely ignored.


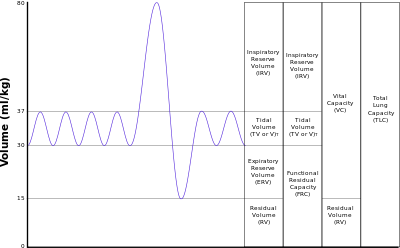 Failure to do so results in atelectasis.
Failure to do so results in atelectasis.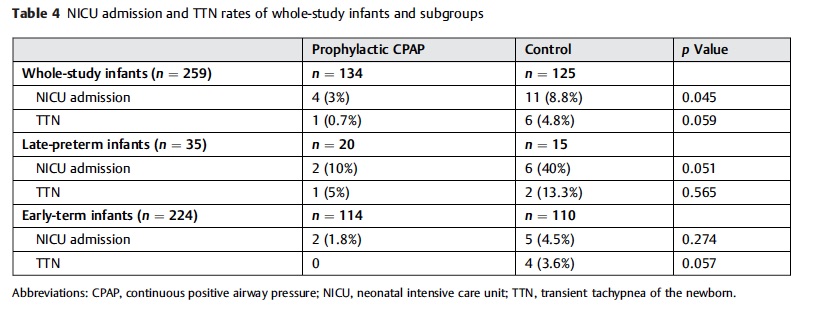 figure. The results here although just achieving significance should not be minimized. Avoiding progressive atelectasis decreases admission rates. The conclusion here is that there is little benefit in adopting a wait and see approach to those kids born by elective c-section. While it is true that you may be treating a significant number of healthy patients between 34 0/7 – 38 6/7 weeks with CPAP it is for a brief period and makes a significant difference in frequency of admission.
figure. The results here although just achieving significance should not be minimized. Avoiding progressive atelectasis decreases admission rates. The conclusion here is that there is little benefit in adopting a wait and see approach to those kids born by elective c-section. While it is true that you may be treating a significant number of healthy patients between 34 0/7 – 38 6/7 weeks with CPAP it is for a brief period and makes a significant difference in frequency of admission.