In an effort to reduce the incidence of IVH many patient care bundles in the last number of years have advocated for minimal handling. As part of approach to minimal handing an effort to keep the head straight and in some centres elevated has been postulated to help with enhancing venous outflow from the head. By reducing the passive gravity aided flow from the brain back into the thorax the theory would be that this would help minimize venous pressure in the draining cerebral system. Lowering pressure would in turn theoretically reduce the risk of IVH and hopefully the most severe types. The evidence to support this practice has largely been observational in the sense that those units practising this sort of intervention have published reductions in rates of severe IVH such as reported for small baby units. The fly in the ointment however is that many changes occur in the care of these infants so definitively attributing the difference in outcomes to just one intervention such as midline head positioning with elevation of the head can be challenging.
A Study to Sort It Out
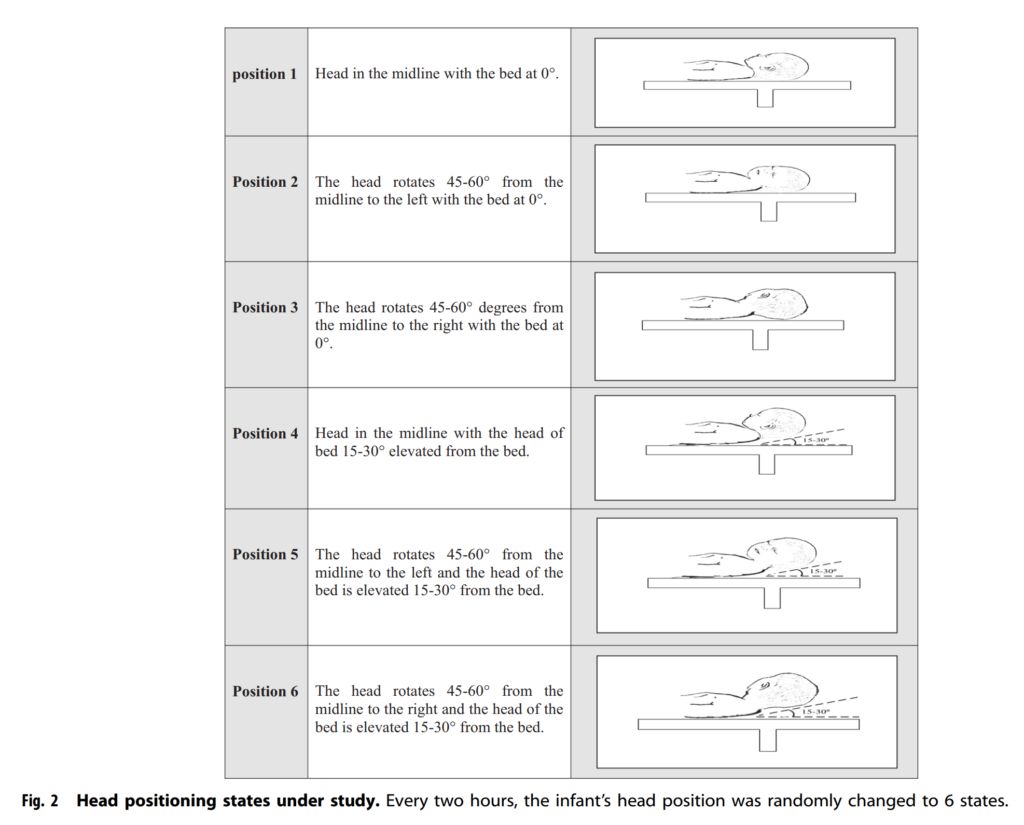
Researchers in Iran sought to answer this question with an elegant study in which 39 patients served as their own controls and had NIRS monitoring through different head positions. This study entitled The effect of head positioning on brain tissue oxygenation in preterm infants: a randomized clinical trial study by Mohamammadie et al looked at these infants over the first 48 hours of life. Each infant went through NIRS monitoring and were randomly placed in six different positions as shown in the figure.
The infants studied were those who would be most vulnerable to IVH so were all <=32 weeks and < 1500g. The authors acknowledged that they would have liked to record over the first 72 hours as this has traditionally become the period of minimal handling in care bundles but claim that they did not have enough data past 48 hours to comment.
Prior to starting positional changes ten minutes of baseline recording was done in the midline position without elevation. Each position was used for a period of 2 hours during which NIRS monitoring was performed. The goal here was to see if the amount of oxygen extraction changed with different head positions and elevations. If the extraction increased in one head position it would be thought to reflect slowed return of venous blood with further extraction of oxygen from the brain.
What did the authors find?
Since I am reporting the findings it shouldn’t surprise you that they found something here. What might surprise you though is the actual difference in what they found. If one would have to guess before sharing the results it would seem that laying the head of the bed flat would not help with venous drainage as much as a 15-30 degree elevation so let’s guess that they would find that. Also, based on a belief that the jugular veins might be kinked if you turn your head to one side or the other let’s guess that midline head positioning does make a difference. Looking at the results below, let’s see if this actually happened.
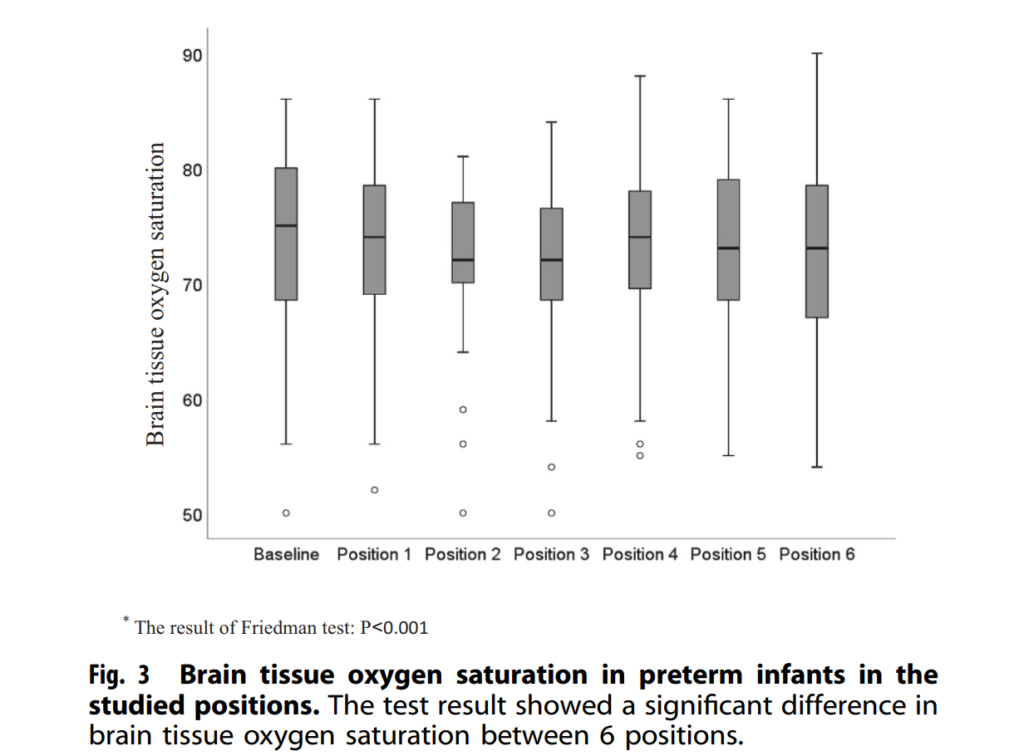
As you can see the highest NIRS recordings were found in the baseline position and in general the three positions with the head of bed elevated (Position 4-6) and when flat in the midline (Position 1). It would seem then that the anticipated benefit was shown! From a statistical standpoint the third position was found to be different as was the fourth compared to the first position.
What does it all mean though?
A statistically different finding was achieved which shows the 3rd and 4th positions are not as good as baseline for sure but what about clinical significance. The lower limit of normal for NIRS readings is about 60. The means for all of these positions were in the 70s. In fact the difference between the mean of the 3rd and 4th positions and the others were only about 2%. Is this enough to make a difference? I honestly am not sure. There is a difference that reaches statistical significance so if we accept that there may have been some disruption of venous flow is this enough evidence to totally explain the reductions in IVH that have been seen with bundles for minimal handling with positioning? There were a lot of variables here that could not be controlled such as time of day that a baby was in one position or another since it was random. Was there a lot of noise in the unit at the time of one position or another? Depending on circadian rhythms what would the cortisol levels be and might mild changes in blood pressure explain the findings since they are so small?
I don’t want to totally dismiss the findings but suspect that it isn’t just the positioning that is leading to reductions in IVH. The same units that promote small baby care are also pushing breastfeeding rates up, skin to skin care and trying to harmonize other aspects of care. If we are seeing reductions in IVH which is a wonderful thing is it all related to this? Probably not but what this study does in my mind is support the theories about enhancing venous drainage through positioning and I see no reason not to continue this practice and try to keep these infants in the mid line and avoid bothering them as much as possible as they transition from the in-utero to ex-utero environment.
I couldn’t think of a better topic for World Prematurity Day 2021 than what constitutes the edge of viability. Thinking back over my career, when I was a resident and fellow infants born at 25 and 26 weeks were deemed about as low as “we should” go but we certainly resuscitated infants at 24 weeks but this was considered heroic. Jump ahead to the last decade and we began caring for infants at birth at 23 weeks so commonly that the thought of offering comfort care only to infants at 24 weeks became almost unthinkable for many health care providers. Before I get jumped on, let me say that I am not saying I agree or disagree with that sentiment but it is something that is felt by many.
The Shared Decision Model
In the last few years a rethink again has occurred whereby the concept of the treating team knowing best has been replaced by the “shared decision model”. In this line of thinking, it is not up to us as health care providers to “tell the parents” what to do but rather come to a shared decision based on an assessment of the wishes and values of the parents in conjunction with hearing about both short and long term problems their infants may face if resuscitated. This concept was central to the statement by the Canadian Pediatric Society that I am proud to have been part of with respect to its development. The statement for those that are interested is Counselling and management for anticipated extremely preterm birth
What’s next? Going below 22 weeks?
The challenge of the shared decision model is that there comes a point where the answer is simply “no”. If for example a family at 19 weeks gestation demanded an attempt at resuscitation I would have to inform them that survival is not possible (assuming ultrasound confirmed anthropometric measurements consistent with that age). The question though becomes a little more difficult to answer at 21 weeks and was the subject of a recent article in the New York Times about a survivor at 21 weeks gestation.
Even with the best gestational age dating the estimate can be off by up to 5 days so it’s possible that the infant in this story was closer to 22 weeks or even midpoint between 22 and 23 weeks in reality. Regardless it does raise the question about what to do at 21 weeks and I suspect we will begin to see more stories about this now that the glass ceiling of 22 weeks has been breached. What about below 21 weeks? Sounds impossible I know but with research that remains at the stage of animal studies this may become possible. Maybe not in the next 5-10 years but it could happen in my lifetime in this chosen field.
The Artificial Placenta
This made headlines a few years ago with the news that the Children’s Hospital of Philadelphia had successfully kept a lamb alive for a period of 4 weeks using an artificial placenta and amniotic fluid.
You might think that this was a one-off experiment that will never see the light of day but similar work is being done in Toronto, Canada where they have been able to do similar work with preterm piglets in their paper Achieving sustained extrauterine life: Challenges of an artificial placenta in fetal pigs as a model of the preterm human fetus. Incidentally as my colleague Dr. Ayman Sheta worked on this project while in Toronto I am particularly pleased to share this research. Similar to the experience in CHOP the team in Toronto has been able to keep piglets alive for progressively longer durations. My understanding is that despite the best efforts infectious complications over arise limiting how long one can sustain such animals.
This leads me to my final thoughts on where we might be able to go. I see a future where we apply such technology to humans but not in the way that people might have thought. Keeping a fetus after delivery at 21 or 20 weeks on an artificial placenta for many weeks is not likely a realistic goal. What if we could get 1 or 2 weeks though and allow the fetus to be oxygenated without using positive pressure on their developing lungs and transition them at 23 or 24 weeks gestation? We may in this way be able to allow for postnatal maturation in a artificial uterine environment and give babies a chance who would otherwise never had the opportunity for a shared decision with medical staff.
Sound like science fiction? Well the beauty of the internet as my friend told me today is that once it’s out there it out there for good. Let’s see how this post stands the test of time and to all the babies out there in NICUs and to their families I wish you all a good and uneventful World Prematurity Day wherever you may be!
The journey from conception to the labour floor and then for some to the NICU is not a straight one. There are times of joy, interspersed with sadness, denial, anger and eventually acceptance, as initial news of being pregnant leads to complications in pregnancy and then eventual admission of an infant to the NICU.
Much has been said in recent years about the building of partnerships with parents and in fact there is a new catchphrase attached to the concept “shared decision making” (SDM). There is no question that in the perfect world this is exactly the relationship that we should be striving for with all of our patients. The world however is not perfect and although this may not be the most popular opinion I have given, I question how applicable this really is in many situations.
A Reality Check
Take for instance the parents who present to the labour floor of their local hospital in advanced labour at 24 weeks. Proponents of this SDM model would suggest that a meeting take place and pertinent information be given to a family and together with the assistance of literature applicable to their situation (possibly a pamphlet) the health care providers and families come to a mutually agreeable decision as to what the best course of action is for them and their unborn infant. This all sounds wonderful but examining the real life situation a little more closely is it actually reasonable to assume we can obtain this? I have not been, nor will I ever be pregnant and certainly have never experienced contractions and felt the veil clouding my vision as the first dose of analgesia enters my veins to deal with the discomfort a woman experiences during labour. Not to mention there are people admitting this couple, taking histories, establishing IV access, scanning bellies and a whole host of other pokes and prods along the way.
My Role Better Defined
Then I come in. Among all this chaos I deliver the information, pass along a pamphlet and do the best job I can to inform said couple of the upcoming decision. The trouble of course is how do we come to this mutual decision in the 15 – 30 minutes I spend with them during this crisis? The answer sadly is we do our best but don’t for a minute think that SDM has occurred. I don’t believe this is possible unless the family has prior experience with a preterm birth or perhaps is a HCP working with newborns or children with disabilities themselves. In fact Boss RD et al in their own research on the subject identified that in hindsight religion, spirituality and hope are what motivated parents rather than what was said at the time. In essence their minds are already made up. It doesn’t mean we shouldn’t strive for the SDM but at least in my opinion, unless their contractions settle, a calmness ensues, they have time to digest the information being given and then meet again under less stressful circumstances, the SDM is a nice idea but for many not a reality.
Shifting To The NICU
I recall a significant moment in my training when I saw how the SDM model can actually cause more grief than help. Dr. Keith Barrington a fellow blogger (if you haven’t discovered him, his work is fascinating over at Neonatal Research) published one of the most impactful pieces of research of the decade during my fellowship. The adverse neuro-developmental effects of postnatal steroids in the preterm infant: a systematic review of RCTs. Following this analysis there was a near moratorium on the use of post natal steroids. The issue this created was that to now receive them you had to be close to the end of the limits of care. At this point you either died (thereby concluding they are of no help) or you survived with disability that was due in part no doubt to how sick you had become (thereby concluding they are dangerous).
The moment I am referring to was a conversation with a family in which the attending managing the unit presented the risks and benefits of postnatal steroids to the family when the FiO2 was at 40% one day. The language used was non directive and the parents asked for another day to decide. The next day and each of the following two days they were unable to choose between giving the steroids and the perceived risk of brain damage versus not and watching the FiO2 climb by about 10% per day. By the time the FiO2 several days later was at 80-90% they were distraught, teary and feeling helpless. What they needed was direction; someone to give them some advice or more simply an educated opinion.
We can strive to share in the decision making but I continue to believe there is a time and place to help our families by taking a stance or side. We can equip them with as much information as we want but is there really any replacement for actually taking care of these infants, experiencing the ups and downs and hearing how they have done in follow-up? We simply can’t expect the average parent to understand the true long term consequences of their decisions. I am not saying we go back to a paternalistic time in medicine but I am saying that one size does not fit all.
We owe it to our families to pursue SDM when we can but we have an equal obligation to recognize when this ideal state is simply not possible. At this point we have to use the experiences and knowledge we have to provide them with the best advice we can. We have gone through medical training, and gone down these paths so many times. We can avoid biased opinion and rely on the facts as they are in our institutions but to not take a stand when it is needed at least for me is doing a disservice to those we are so eager to help.
In the book Outliers by Malcolm Gladwell he talked about 10000 hours being the threshold at which if you practiced or gained that much experience with something you could become an expert. In Sweden the approach to 22 week pregnancies and above is to resuscitate all as a strategy. I wrote about this before in At 22 weeks of gestation does your faith matter most to outcome? The information gleaned from that paper was that if you have a policy of resuscitation at these gestational ages and you compare outcomes to a centre that is selective in who they resuscitate the outcomes are better when you believe all should be resuscitated.
New Study Expands Data
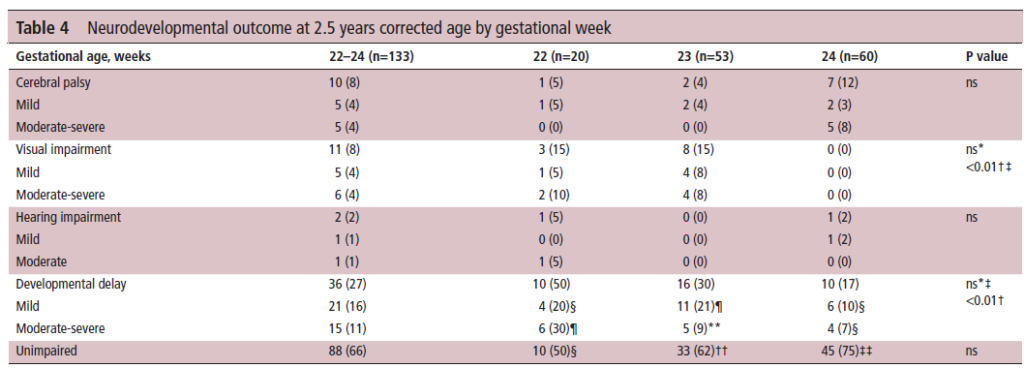
The same group has published this time around the results of the same cohort from 2006-2015 but this time with developmental outcome data. The paper is entitled Outcomes of a uniformly active approach to infants born at 22-24 weeks of gestation In this paper they discuss outcomes at 234 and 24 weeks respectively in addition to the findings for 22 weeks which they covered in the paper mentioned above. The reason for sharing this study is that if I asked you to imagine going into a room right now and talking to a family at 22 – 24 weeks and predicting the outcome of their infant, my hunch is that you would not provide as rosy a picture as the group in Uppsala, Sweden.
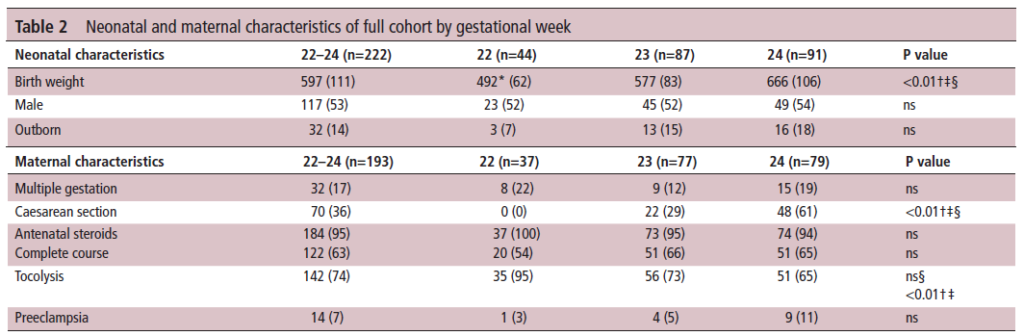
The authors looked at a group of infants with the following breakdown by gestational age.
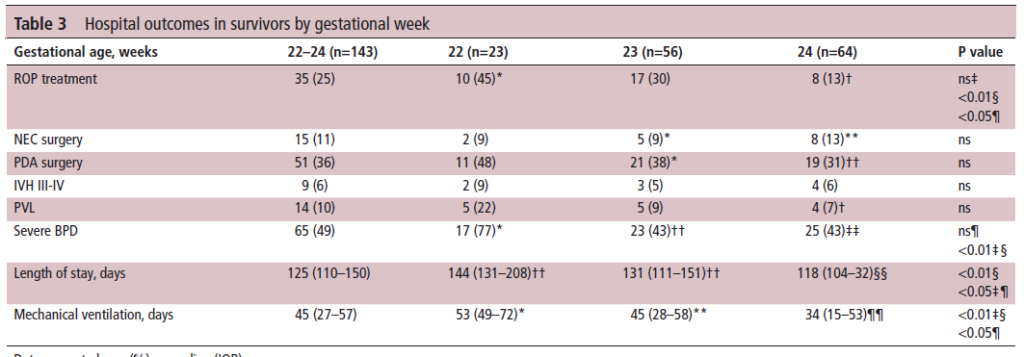
Not surprisingly as gestational age declines the incidence of complications rise but looking at Table 3 even at 22 weeks there was no difference in rate of NEC or need for PDA surgery. Nor was there a difference in rates of severe IVH/PVL. Rates of BPD were higher and likely attributable to the longer durations of positive pressure ventilation. Are these rates for these complications terrible though when the other option is non-intervention which for certain means death?
What about outcome?
Looking at the outcome at 2.5 years, the rate of cerebral palsy is about 1:10 to 1:20 for all GA. Hearing impairment is almost non-existent and while developmental delay is detected in 50 percent of survivors at 22 weeks only about a quarter of the infants have severe impairment.
Deciding what to do
There is no question that many of you seeing what this post was about would simply say “NO WAY” but in the end isn’t it really about a shared decision with the family? It wasn’t that long ago that we had to have a real paradigm shift in thinking about resuscitating 23 week infants. The amount of mental energy spent for teams worldwide coming to this decision was tremendous and now if you were to suggest compassionate care at 24 weeks you get a look back like you are crazy! It wasn’t that long ago that 24 weeks was considered viability in many places and now that 23 is the new 24 this is the struggle some people have now. Should we go to 22 weeks everywhere as the Swedes have? Clearly this is a decision that institutions need to look at critically and determine if they have the space to accomodate. Each infant should they survive will occupy a bed for at least 6 months. This needs to be looked at before one can just say sure this is a good idea.
In the end what the study demonstrates I believe is that the outcome at 22 and 23 weeks for that matter need not be universally dismal. There certainly is a good chance that a surviving infant will have one or more deficits but in the end I would advocate this is a conversation all units need to be having and critically look at whether each institution has the capactity to consider.
My bet is that five years from now this discussion will be moot as we will be mostly in that direction but at this time I think we are still in evolution.
It has been a few months now that I have been serving as Chair of the Fetus and Newborn Committee for the Canadian Pediatric Society. Certain statements that we release resonate strongly with me and the one just released this week is certainly one of them. Guidelines for vitamin K prophylaxis in newborns is an important statement about a condition that thankfully so few people ever experience. To read the statement on the CPS website click here.
Similar story to vaccinations
Prior to the American Academy of Pediatrics in 1961 proclaiming that all newborns should receive IM Vitamin K at birth the incidence of Vitamin K deficient bleeding was 0.25 – 1.7%. Think about that for a moment. A new parent could expect that 1/100 babies roughly might have intestinal bleeding or worse an intracranial hemorrhage due to an insufficient amount of vitamin K levels in the newborn. The types of bleeding could be categorized into three different time epochs. Early onset (occurring in the first 24 hours post-birth), classic (occurring at days 2 to 7) and late onset (at 2 to 12 weeks and up to 6 months of age).
With a rate that high detractors of providing Vitamin K at birth would say “why should we give it; I haven’t heard of any baby getting such bleeding?” Looking at it another way though, why don’t you see congenital rubella or kids with measles much these days? It’s due to vaccination. Thankfully as a Neonatologist, I don’t see Vitamin K deficient bleeding since most parents provide Vitamin K to their babies at birth. If you went back to the era prior to 1961 when widespread supplementation of Vitamin K began in the US, I imagine it would not have been too uncommon to hear about a baby who had bleeding issues after birth. Just because we don’t hear about German Measles much anymore doesn’t mean the virus causing it doesn’t still exist!
How Effective is Vitamin K?
How effective is Vitamin K administration at birth in preventing hemorrhagic disease of the newborn (HDNB)? Studies estimate an incidence of 0.25 per 100000 live births or 1 in 400000 babies vs the 1/100 risk without any vitamin K. That is one effective intervention! At this point I would ask those families that are still concerned about giving Vitamin K to their infants if this is a risk they can accept? If they refuse Vitamin K and there is a significant bleed how will they react?
The Change in this CPS Statement From the Past
In the last statement on Vitamin K, the authors suggested that the oral route was a reasonable option. Instead of giving 1 mg of Vitamin K IM one would dose it as 2 mg orally and then repeat at 2-4 weeks and then 6-8 weeks. In looking at the effectiveness though it is worth noting that while we can assure that families will get the first dose, as with any medication that needs repeat dosing there is the risk of forgetfulness leading to missed dosing down the road. In fact when the authors looked at the risk of late HDNB they found the following “The relative risk for VKDB, when comparing PO versus IM vitamin K administration in these two studies, was 28.75 (95% CI 1.64 to 503.45) and 5.97 (95% CI 0.54 to 65.82), respectively [19][20].”
The outcome of course remains rare but the risk based on two studies was almost 30 times higher than if IM dosing was given.
On this basis IM is recommended.
Having said all this I recognize that despite all this information, some families will choose for a number of reasons to still opt for the oral dose. As the statement suggests we need to encourage such use when a family refuses IM vitamin K. The 30 fold risk compared to IM administration is magnitudes lower than the approximate 1/100 risk of giving nothing at all!
In the end I believe that one case of intracranial hemorrhage from inadequate vitamin K is too much. This one vitamin indeed could save a life.
A few weeks back I wrote about the topic of intubations and whether premedication is really needed (Still performing awake intubations in newborns? Maybe this will change your mind.) I was clear in my belief that it is and offered reasons why. There is another group of practitioners though that generally agree that premedication is beneficial but have a different question. Many believe that analgesia or sedation is needed but question the need for paralysis. The usual argument is that if the intubation doesn’t go well and the patient can’t spontaneously ventilate could we be worse off if the patient loses their muscle tone.
Neonatal Intubation Registry
At the CPS meeting last month in Quebec City. I had the pleasure of listening to a talk by Dr. Elizabeth Foglia on the findings from a Neonatal intubation registry that many centres have been contributing to. The National Emergency Airway Registry for Neonates (NEAR4NEOs), records all intubations from a number of centres using an online database and allows for analysis of many different aspects of intubations in neonates.
This year, J. Krick et al published Premedication with paralysis improves intubation success and decreases adverse events in very low birth weight infants: a prospective cohort study. This study compared results from the registry of two centres, the University of Washington Medical Center (UWMC) and Seattle Children’s Hospital where the former rarely uses paralysis and the latter in almost all instances of non-emergent intubation. In all, 237 encounters were analyzed in the NICU for babies < 1500g with the majority of encounters (181) being from UWMC. The median PMA at intubation was 28 completed weeks (IQR: 27, 30), chronological age was 9 days (IQR: 2, 26) and weight was 953 g (IQR: 742,1200). The babies were compared based on the following groups. Premedication with a paralytic 21%, without a paralytic 46% and no premedication 31%.
This was an observational study that examined the rates of adverse events and subdivided into severe (cardiac arrest, esophageal intubation with delayed recognition, emesis with witnessed aspiration, hypotension requiring intervention (fluid and/or vasopressors), laryngospasm, malignant hyperthermia, pneumothorax/pneumomediastinum, or direct airway injury) vs non-severe (mainstem bronchial intuba- tion, esophageal intubation with immediate recognition, emesis without aspiration, hypertension requiring therapy, epistaxis, lip trauma, gum or oral trauma, dysrhythmia, and pain and/or agitation requiring additional medication and causing a delay in intubation.).
How did the groups compare?
It turns out paralysis seems to be a big deal (at least in this group of infants). Use of paralysis resulted in less attempts to intubate (median 1 attempt; IQR: 1, 2.25 vs. 2; IQR: 1, 3, p < 0.05)). In fact success was no different between the groups with no paralysis or no premedication at all! When it comes to tracheal intubation adverse events the impact of using paralysis becomes more evident. Paralysis does make a difference in reducing the incidence of such events and moreover when only looking at the rate of severe adverse events as defined above the finding was that none occurred when paralysis was used vs 9 when no paralysis was employed and 5 when no premedication was used at all. The rate of bradycardic events was less in the paralytic group but rates of oxygen desaturation between the three arms were no different.
How do we interpret the results?
Based on the results from the registry it looks like paralysis is a good thing here when electively intubating infants. If we try to determine the reason for it I suspect it may have much to do with the higher likelihood of success on the first attempt at placing an ETT. The longer it takes to place the ETT or the more number of attempts requiring intermittent PPV in a patient who truly needs a tube the greater the likelihood that you will see adverse events including bradycardia. It may simply be that a calm and still patient is an easier intubation and getting the tube in faster yields a more stable patient.
I am biased though and I think it is worth pointing out another possible reason for the differing results. One hospital in this study routinely used premedication and the other did not. Almost 3/4 of the patients came from one hospital which raises the possibility that skill set could be playing a role. If the skill of providers at the two hospitals differed, the results could reflect the variable skill in the practitioners versus the difference in the medications used themselves. What I don’t know though is whether the two share the same training program or not. Are the trainees the same at both sites (google maps says the two sites are 11 minutes away by car)? The difference still might be in local respiratory therapists or Neonatologists intubating as well. Regardless, the study provides evidence that paralysis makes a difference. To convince those out there though who remain skeptical I think we are going to need the registry to take part in a prospective trial using many centres. A format in which several centres that don’t use paralysis are compared to several who do routinely would help to sort out the concern in skill when looking only at two centres. This wouldn’t be randomized of course but I think it would be very difficult at this point to get a centre that strongly believes in using paralysis to randomize so a prospective study using groups chosen by the individual centre might be the next best thing. If anyone using the registry is reading this let me know what you think?





 I am not saying we go back to a paternalistic time in medicine but I am saying that one size does not fit all.
I am not saying we go back to a paternalistic time in medicine but I am saying that one size does not fit all.



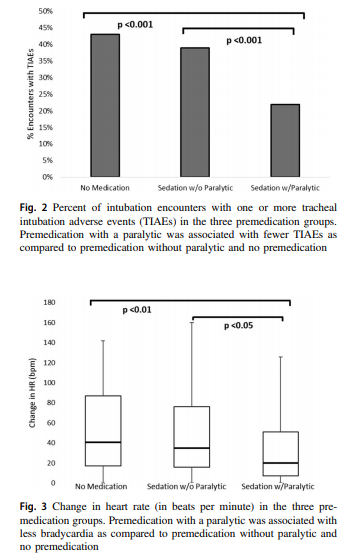 Paralysis does make a difference in reducing the incidence of such events and moreover when only looking at the rate of severe adverse events as defined above the finding was that none occurred when paralysis was used vs 9 when no paralysis was employed and 5 when no premedication was used at all. The rate of bradycardic events was less in the paralytic group but rates of oxygen desaturation between the three arms were no different.
Paralysis does make a difference in reducing the incidence of such events and moreover when only looking at the rate of severe adverse events as defined above the finding was that none occurred when paralysis was used vs 9 when no paralysis was employed and 5 when no premedication was used at all. The rate of bradycardic events was less in the paralytic group but rates of oxygen desaturation between the three arms were no different.