The lungs of a preterm infant are so fragile that over time pressure limited time cycled ventilation has given way to volume guaranteed (VG) or at least measured breaths. It really hasn’t been that long that this has been in vogue. As a fellow I moved from one program that only used VG modes to another program where VG may as well have been a four letter word. With time and some good research it has become evident that minimizing excessive tidal volumes by controlling the volume provided with each breath is the way to go in the NICU and was the subject of a Cochrane review entitled Volume-targeted versuspressure-limited ventilation in neonates. In case you missed it, the highlights are that neonates ventilated with volume instead of pressure limits had reduced rates of:
death or BPD
pneumothoraces
hypocarbia
severe cranial ultrasound pathologies
duration of ventilation
These are all outcomes that matter greatly but the question is would starting this approach earlier make an even bigger difference?
Volume Ventilation In The Delivery Room
I was taught a long time ago that overdistending the lungs of an ELBW in the first few breaths can make the difference between a baby who extubates quickly and one who goes onto have terribly scarred lungs and a reliance on ventilation for a protracted period of time. How do we ventilate the newborn though? Some use a self inflating bag, others an anaesthesia bag and still others a t-piece resuscitator. In each case one either attempts to deliver a PIP using the sensitivity of their hand or sets a pressure as with a t-piece resuscitator and hopes that the delivered volume gets into the lungs. The question though is how much are we giving when we do that?
High or Low – Does it make a difference to rates of IVH?
One of my favourite groups in Edmonton recently published the following paper; Impact of delivered tidal volume on the occurrence of intraventricular haemorrhage in preterm infants during positive pressure ventilation in the delivery room. This prospective study used a t-piece resuscitator with a flow sensor attached that was able to calculate the volume of each breath delivered over 120 seconds to babies born at < 29 weeks who required support for that duration. In each case the pressure was set at 24 for PIP and +6 for PEEP. The question on the authors’ minds was that all other things being equal (baseline characteristics of the two groups were the same) would 41 infants given a mean volume < 6 ml/kg have less IVH compared to the larger group of 124 with a mean Vt of > 6 ml/kg. Before getting into the results, the median numbers for each group were 5.3 and 8.7 mL/kg respectively for the low and high groups. The higher group having a median quite different from the mean suggests the distribution of values was skewed to the left meaning a greater number of babies were ventilated with lower values but that some ones with higher values dragged the median up.
Results
IVH
< 6 mL/kg
> 6 ml/kg
p
1
5%
48%
2
2%
13%
3
0
5%
4
5%
35%
Grade 3 or 4
6%
27%
0.01
All grades
12%
51%
0.008
Let’s be fair though and acknowledge that much can happen from the time a patient leaves the delivery room until the time of their head ultrasounds. The authors did a reasonable job though of accounting for these things by looking at such variables as NIRS cerebral oxygenation readings, blood pressures, rates of prophylactic indomethacin use all of which might be expected to influence rates of IVH and none were different. The message regardless from this study is that excessive tidal volume delivered after delivery is likely harmful. The problem now is what to do about it?
The Quandary
Unless I am mistaken, there isn’t a volume regulated bag-mask device that we can turn to for control of delivered tidal volume. Given that all the babies were treated the same with the same pressures I have to believe that the babies with stiffer lungs responded less in terms of lung expansion so in essence the worse the baby, the better they did in the long run at least from the IVH standpoint. The babies with the more compliant lungs may have suffered from being “too good”. Getting a good seal and providing good breathes with a BVM takes a lot of skill and practice. This is why the t-piece resuscitator grew in popularity so quickly. If you can turn a couple of dials and place it over the mouth and nose of a baby you can ventilate a newborn. The challenge though is that there is no feedback. How much volume are you giving when you start with the same settings for everyone? What may seem easy is actually quite complicated in terms of knowing what we are truly delivering to the patient. I would put to you that someone far smarter than I needs to develop a commercially available BVM device with real-time feedback on delivered volume rather than pressure. Being able to adjust our pressure settings whether they be manual or set on a device is needed and fast!
Perhaps someone reading this might whisper in the ear of an engineer somewhere and figure out how to do this in a device that is low enough cost for everyday use.
We can always learn and we can always do better. At least that is something that I believe in. In our approach to resuscitating newborns one simple rule is clear. Fluid must be replaced by air after birth and the way to oxygenate and remove CO2 is to establish a functional residual capacity. The functional residual capacity is the volume of air left in the lung after a tidal volume of air is expelled in a spontaneously breathing infant and is shown in the figure. Traditionally, to establish this volume in a newborn who is apneic, you begin PPV or in the spontaneously breathing baby with respiratory distress provide CPAP to help inflate the lungs and establish FRC.
Is there another way?
Something that has been discussed now for some time and was commented on in the most recent version of NRP was the concept of using sustained inflation (SI) to achieve FRC. I have written about this topic previously and came to a conclusion that it wasn’t quite ready for prime time yet in the piece Is It Time To Use Sustained Lung Inflation In NRP?
The conclusion as well in the NRP textbook was the following:
“There are insufficient data regarding short and long-term safety and the most appropriate duration and pressure of inflation to support routine application of sustained inflation of greater than 5 seconds’ duration to the transitioning newborn (Class IIb, LOE B-R). Further studies using carefully designed protocols are needed”
So what now could be causing me to revisit this concept? I will be frank and admit that whenever I see research out of my old unit in Edmonton I feel compelled to read it and this time was no different. The Edmonton group continues to do wonderful work in the area of resuscitation and expand the body of literature in such areas as sustained inflation.
Can you predict how much of a sustained inflation is needed?
This is the crux of a recent study using end tidal CO2 measurement to determine whether the lung has indeed established an FRC or not. Dr. Schmolzer’s group in their paper (Using exhaled CO2 to guide initial respiratory support at birth: a randomised controlled trial) used end tidal CO2 levels above 20 mmHg to indicate that FRC had been established. If you have less CO2 being released the concept would be that the lung is actually not open. There are some important numbers in this study that need to be acknowledged. The first is the population that they looked at which were infants under 32 6/7 weeks and the second is the incidence of BPD (need for O2 or respiratory support at 36 weeks) which in their unit was 49%. This is a BIG number as in comparison for infants under 1500g our own local incidence is about 11%. If you were to add larger infants closer to 33 weeks our number would be lower due to dilution. With such a large number though in Edmonton it allowed them to shoot for a 40% reduction in BPD (50% down to 30%). To accomplish this they needed 93 infants in each group to show a difference this big.
So what did they do?
For this study they divided the groups in two when the infant wouldn’t breathe in the delivery room. The SI group received a PIP of 24 using a T-piece resuscitator for an initial 20 seconds. If the pCO2 as measured by the ETCO2 remained less than 20 they received an additional 10 seconds of SI. In the PPV group after 30 seconds of PPV the infants received an increase of PIP if pCO2 remained below 20 or a decrease in PIP if above 20. In both arms after this phase of the study NRP was then followed as per usual guidelines.
The results though just didn’t come through for the primary outcome although ventilation did show a difference.
Outcome
SI
PPV
p
BPD
23%
33%
0.09
Duration of mechanical ventilation (hrs)
63
204
0.045
The reduction in hours of ventilation was impressive although no difference in BPD was seen. The problem though with all of this is what happened after recruitment into the study. Although they started with many more patients than they needed, by the end they had only 76 in the SI group and 86 in the PPV group. Why is this a problem? If you have less patients than you needed based on the power calculation then you actually didn’t have enough patients enrolled to show a difference. The additional compounding fact here is that of the Hawthorne Effect. Simply put, patients who are in a study tend to do better by being in a study. The observed rate of BPD was 33% during the study. If the observed rate is lower than expected when the power calculation was done it means that the number needed to show a difference was even larger than the amount they originally thought was needed. In the end they just didn’t have the numbers to show a difference so there isn’t much to conclude.
What I do like though
I have a feeling or a hunch that with a larger sample size there could be something here. Using end tidal pCO2 to determine if the lung is open is in and of itself I believe a strategy to consider whether giving PPV or one day SI. We already use colorimetric devices to determine ETT placement but using a quantitative measure to ascertain the extent of open lung seems promising to me. I for one look forward to the continued work of the Neonatal Resuscitation–Stabilization–Triage team (RST team) and congratulate them on the great work that they continue doing.
I know how to bag a baby. At least I think I do. Providing PPV with a bag-valve mask is something that you are taught in NRP and is likely one of the first skills you learned in the NICU. We are told to squeeze the bag at a rate of 40-60 breaths a minute. According to the Laerdal website, the volume of the preterm silicone bag that we typically use is 240 mL. Imagine then that you are wanting to ventilate a baby who is 1 kg. How much should you compress the bag if you wish to delivery 5 mL/kg. Five ml out of a 240 mL bag is not a lot of squeeze is it? Think about that the next time you find yourself squeezing one. You might then say but what about a t-piece resuscitator? A good choice option as well but how much volume are you delivering if you set the initial pressures at 20/5 for example? That would depend on the compliance of the lung of course. The greater the compliance the more volume would go in. Would it be 5 mL, 10 ml or even 2.5 mL based on the initial setting? Hard to say as it really depends on your seal and the compliance of the lung at the pressure you have chosen. If only we had a device that could deliver a preset volume just like on a ventilator with a volume guarantee setting!
Why is this holy grail so important?
It has been over 30 years since the importance of volutrauma was demonstrated in a rabbit model. Hernandez LA et al published Chest wall restriction limits high airway pressure-induced lung injury in young rabbits. The study used three models to demonstrate the impact of volume as opposed to pressure on injuring the lung of preterm rabbits. Group 1 were rabbit ventilated at pressures of 15/30/45 cm H2O for one hour, group 2 rabbits with a cast around their thorax to limit volume expansion and group 3 sets of excised lungs with no restriction to distension based on the applied pressures. As you might expect, limitation of over distension by the plaster cast led the greatest reduction in injury (measured as microvascular permeability) with the excised lungs being the worst. In doing this study the authors demonstrated the importance of over distension and made the case for controlling volume more than pressure when delivering breaths to avoid excessive tidal volume and resultant lung injury.
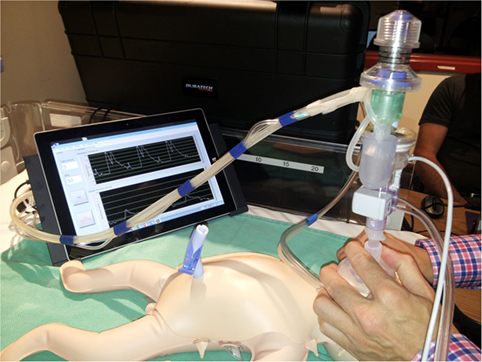
The “Next Step” Volume Ventilator BVM
Perhaps I am becoming a fan of the Edmonton group. In 2015 they published A Novel Prototype Neonatal Resuscitator That Controls Tidal Volume and Ventilation Rate: A Comparative Study of Mask Ventilation in a Newborn Manikin. The device is tablet based and as described, rather than setting a PIP to deliver a Vt, a rate is set along with a volume to be delivered with a peep in this case set at +5. This study compared 5 different methods of delivering PPV to a 1 kg preterm manikin. The first was a standard self inflating bag, the next three different t-piece resuscitators and then the Next Step. For the first four the goal was to deliver a pressure of 20/5 at a rate of 40-60 breaths per minute. A test lung was connected to the manikin such that each device was used for a one minute period at three different levels of compliance (0.5 ml/cmH2O, 1.0 ml/cmH2O and then 2.0 ml/cm H2O representing increasing compliance. The goal of the study was to compare the methods in terms of delivering a volume of 5 mL to this 1 kg model lung. The order in which the devices were used was randomized for the 25 participants in the study who were all certified in NRP and included some Neonatologists.
Some Concerning Findings
As I said at the beginning, we all like to think we know how to ventilate a newborn with BVM. The results though suggest that as compliance increases our ability to control how much volume we deliver to a lung based on a best guess for pressures needed is lacking. One caveat here is that the pressures set on the t-piece resucitators were unchanged during the 1 minute trials but then again how often during one minute would we change settings from a starting point of 20/5?
Vt (mL)
0.5 mL/cmH20
1.0 mL/cmH20
2.0mL/cmH20
Self inflating
11.4
17.6
23.5
Neo-Tee
5.6
11.2
19.3
Neopuff
6.1
10
21.3
Giraffe
5.7
10.9
19.8
Next Step
3.7
4.9
4.5
Without putting in all the confidence intervals I can tell you that the Next Step was the tightest. What you notice immediately (or at least I did) was that no matter what the compliance, the self inflating bag delivers quite an excessive volume even in experienced hands regardless of compliance. At low compliance the t-piece resuscitators do an admirable job as 5-6 ml/kg of delivered Vt is reasonable but as compliance improves the volumes increase substantially. It is worth pointing out that at low compliance the Next Step was unable to deliver the prescribed Vt but knowing that if you had a baby who wasn’t responding to ventilation I would imagine you would then try a setting of 6 ml/kg to compensate much like you would increase the pressure on a typical device. How might these devices do in a 29 week infant for example with better compliance than say a 24 week infant? You can’t help but wonder how many babies are given minutes of excessive Vt after birth during PPV with the traditional pressure limited BVM setup and then down the road how many have BPD in part because of that exposure.
I wanted to share this piece as I think volume resuscitation will be the future. This is just a prototype or at least back then it was. Interestingly in terms of satisfaction of use, the Next Step was rated by the participants in the study as being the easiest and most comfortable to use of all the devices studied. Adding this finding to the accuracy of the delivered volume and I think we could have a winner.
Things aren’t the way they used to be. When I was training, opportunities abounded for opportunities to intubate infants. Then we did away with intubating vigourous infants born through meconium and now won’t be electively intubating them at all. Then you can add in the move towards use of non-invasive respiratory support instead of intubating and giving surfactant and voila…you have the perfect barrier for training residents and others how to intubate. On top of all of this the competition for learning has increased as the skill that was once the domain of the physician has now spread (quite rightly) to respiratory therapists, nurses in some places and with the growth of residency programs (ours is now 2.5X larger than when I trained) the scarce chances are divided among many.
Enter the Video Laryngoscope
To be clear this isn’t a post to promote a product but rather an examination of the effectiveness of a tool. I am putting this out there recognizing the possibility that someone out there might have heard of or have been contemplating purchasing one of these items. Those that are quite proficient at intubation (likely trained in the “good old days”) would likely question the need for such a device but I believe the device isn’t really aimed at that group except to use perhaps as a teaching tool. It really is targeted (at least I think) for those who don’t perform the skill often.
Does use of the video laryngoscope improve success rates at intubation?
This question has had an attempt now at being answered by Parmekar S et al in their paper Mind the gap: can videolaryngoscopy bridge the competency gap in neonatal endotracheal intubation among pediatric trainees? a randomized controlled study. The study involved taking 100 pediatric residents and randomizing them into two groups. The first would use the videolaryngoscope (VL group) and then intubate using the standard technique of direct laryngoscopy (DL group). The second group started with DL and then changed to VL. Both groups took part in a training session on intubation and then participated in three simulation scenarios from NRP. The findings demonstrated a couple interesting things. The first as shown in the graph was that the group that started with the laryngoscope had a near 90% success rate compared to about 60% for the traditional approach. When the groups swapped though they were both equal in effectiveness. This suggests that by visualizing the airway with the VL students were able to identify structures better after doing so such that success was improved simply by having used the device.
The other finding worth mentioning was that when the times to intubation were looked at, there was no difference between the two groups at all. If the intubation success is no different, why might the times be the same? Having used the video laryngoscope myself it does take some getting used to. Rather than looking directly at the airway you find yourself looking off to the side and adjusting the approach that is in front of you to place the ETT. No doubt this does take some getting used to.
What I would have liked to see is a repeat assessment a week later after using a few more trials with the VL as I suspect once you are used to it the speed of intubation would improve as well. I suppose though we will have to wait a little while until someone does such work but as a means of improving success in intubation I believe this tool has something to add.
Look around you. Technology is increasingly becoming pervasive in our everyday lives both at home and at work. The promise of technology in the home is to make our lives easier. Automating tasks such as when the lights turn on or what music plays while you eat dinner (all scripted) are offered by several competitors. In the workplace, technology offers hopes of reducing medical error and thereby enhancing safety and accuracy of patient care. The electronic health record while being a nuisance to some does offer protection against incorrect order writing since the algorithms embedded in the software warn you any time you stray. What follows is a bit of a story if you will of an emerging technology that has caught my eye and starts like many tales as a creative idea for one purpose that may actually have benefits in other situations.
Meet Stethocloud
In 2012 students in Australia rose to the challenge and designed a digital stethoscope that could be paired with a smartphone. The stethoscope was able to send the audio it was receiving to the smartphone for analysis and provide an interpretation. The goal here was to help diagnose childhood pneumonia with a stethoscope that would be affordable to the masses, even “Dr. Mom” as the following video documents. Imagine before calling your health line in your city having this $20 tool in your hands that had already told you your child had breath sounds compatible with pneumonia. Might help with moving you up the triage queue in your local emergency department.
Shifting the goal to helping with newborns
Of course breath sounds are not the only audio captured in a stethoscope. Heart sounds are captured as well and the speed of the beats could offer another method of confirming the heart is actually beating. Now we have ECG, pulse oximetry, auscultation and palpation of the umbilical stump to utilize as well so why do you need another tool? It comes down to accuracy. When our own heart rates are running high, how confident are we in what we feel at the stump (is that our own pulse we are feeling?). In a review on measurement of HR by Phillipos E et al from Edmonton, Alberta, auscultation was found to take an average of 17 seconds to produce a number and in 1/3 of situations was incorrect. The error in many cases would have led to changes in management during resuscitation. Palpation of the umbilical cord is far worse. In one study “cord pulsations were impalpable at the time of assessment in 5 (19%) infants, and clinical assessment underestimated the ECG HR with a mean (SD) difference between auscultation and palpation and ECG HR of − 14 (21) and − 21 (21) beats min –1″. In another study, 55% of the time providers were incorrect when they thought the HR was under 100 BPM. This leaves the door open for something else. Might that something be the digital stethoscope?
How does the digital stethoscope fare?
Kevac AC et al decided to look at the use of the Stethocloud to measure HR after birth in infants >26 weeks gestational age at birth. The opted to use the ECG leads as the gold standard which arguably is the most accurate method we have for detecting HR. The good news was that the time to signal acquisition was pretty impressive. The median time to first heart rate with the stethoscope was 2 secs (IQR 1-7 seconds). In comparison the time for a pulse oximeter to pick up HR is variable but may be as long as one minute. In low perfusion states it may be even longer or unable to pick up a good signal. The bad news was the accuracy as shown in the Bland Altman plot. The tendency of the stethoscope was to underestimate the EKG HR by about 7 BPM. Two standard deviations though had it underestimate by almost 60 BPM or overestimate by about 50 BPM. For the purposes of resuscitation, this range is far to great. The mean is acceptable but the precision around that mean is to wide. The other issue noted was the frequent missing data from loss of contact with the patient. Could you imagine for example having a baby who has a heart rate of 50 by the stethoscope but by EKG 100? Big difference in approach, especially if you didn’t have EKG leads on to confirm. The authors note that the accuracy is not sufficient and felt that an improvement in the software algorithms might help.
Another go at it
So as suggested, the same group after having a new version with improved software decided to go at it again. This time Gaertner VD et al restricted the study to term infants. Forty four infants went through the same process again with the stethoscope output being compared to EKG lead results. This time around the results are far more impressive. There was virtually no difference between the ECG and the stethoscope with a 95% confidence interval as shown in the graphs with A being for all recordings and B being those without crying (which would interfere with the acquiring of HR). A maximal difference of +/- 18 BPM for all infants is better than what one gets with auscultation or palpation in terms of accuracy and let’s not forget the 2 second acquisition time!
Should you buy one?
I think this story is evolving and it wouldn’t surprise me if we do see something like this in our future. It certainly removes the element of human error from measuring. It is faster to get a signal than even the time it takes to get your leads on. Where I think it may have a role though is for the patient who has truly no pulse. In such a case you can have an EKG HR but the patient could be in pulseless electrical activity. Typically in this case people struggle to feel a pulse with the accuracy being poor in such situations. Using a device that relies on an actual heart contraction to make a sound provides the team with real information. Concurrent with this technology is also the rise of point of care ultrasound which could look at actual cardiac contractions but this requires training that makes it less generalizable. Putting a stethoscope on a chest is something we all learn to do regardless of our training background.
I think they could be on to something here but perhaps a little more evidence and in particular a study in the preterm infant would be helpful to demonstrate similar accuracy.
I think my first training in resuscitation began with the principles outlined in the NRP 3rd edition program. As we have moved through subsequent editions with the current edition being number 7, I can’t help but think about how many changes have occurred over that time. One such change has been the approach to using medications as part of a resuscitation. Gone are such things as calcium gluconate, naloxone and sodium bicarbonate but something that has stood the test of time is epinephrine. The dosing and recommendations for administering epinephrine have changed over time as well with the dose of endotracheal medication increasing from 0.01 to 0.03 and now to 0.05 – 0.1 mg/kg. While this dosing has increased, that of IV administration has remained the same at 0.01 to 0.03 mg/kg. The change in dosing for the ETT route was due to an increasing awareness that this route just isn’t as effective as IV. Having said that with only 0.1% of resuscitations requiring such support the experience with either route is fairly limited.
What is the concern?
Giving a medication directly via the IV route ensures the dose reaches the heart in the amount desired. In the case of ETT administration there are a few potential issues along the way. The first is that one needs to push the dose down the ETT and this presumes the ETT is actually in the trachea (could have become dislodged). Secondly, if the medication is sent to the lung what effect does the liquid component in the airways have in terms of dilution and distribution of the medication? Lastly, even if you get the epinephrine to the lung it must be picked up at the capillary level and then returned to the left side of the heart. In the absence of significant forward pulmonary blood flow this is not assured.
What is the evidence?
In terms of human clinical research it remains fairly limited. Barber published a retrospective review of 47 newborns who received epinephrine via the endotracheal route. The study Use and efficacy of endotracheal versus intravenous epinephrine during neonatal cardiopulmonary resuscitation in the delivery room found that spontaneous circulation was restored in 32% of this cohort. Following the first dose, a subsequent dose of intravenous epinephrine restored circulation in 77%. This study provided the first suggestion that the IV route may be better than endotracheal. Keep in mind though that this study was retrospective and as the authors conclude in the end, prospective studies are needed to confirm these findings. The question really is what is the likelihood of restoring circulation if the first dose is given IV?
Eleven years later we have a second study that attempts to answer this question although once again it is retrospective. Efficacy of Intravenous and Endotracheal Epinephrine during NeonatalCardiopulmonary Resuscitation in the Delivery Room by Halling et al. This study really was designed to answer two questions. The study group looked at the period from July 2006 to July 2014. During this period the dose of IV epinephrine remained unchanged as per NRP recommendations but the dose of endotracheal epinephrine increased from 0.01 to 0.03 and then to 0.05 mg/kg endotracheally. The increase was in response to both NRP and site observations that the lower doses were not achieving the effect they were hoping for.
The Results
ETT epinephrine
IV Epinephrine
Number
30
20
Return of circulation
23
15
1 dose
6
4
2 dose
5
8
3 doses
9
0
4 doses
3
3
In the ETT group all doses except for 3 after the first dose were given as IV. There was no difference in the response rate over time suggesting that higher doses do not truly increase the chance of a better response. The authors noted that the effectiveness of the two arms were not that different despite a significantly higher dose of epinephrine being administered to the group receiving ETT epinephrine first which is not surprising given the higher recommended dosages.
What I find interesting though is that giving the first dose of epinephrine was given IV in 20 of the paitents, if it is indeed the better route one might expect a better response than in the ETT group. The response from one dose of ETT epi was 20% while that from the IV first group was in fact also only 20%! We do indeed need to be careful here with small numbers but the results at least to me do not suggest strongly that giving IV epi first ensures success. What the study suggests to me is that two doses of epinephrine may be needed to restore circulation. If you choose to start with IV it certainly does not seem unwise but if you have any delays I don’t see any reason to avoid ETT epinephrine as your first line.
The reality is that for many individuals a UVC is a procedure that while they may have learned in an NRP class they may have never actually placed one. Having an ETT in place though seems like a good place to start. I doubt we will ever see a randomized trial of ETT vs IV epinephrine in Neonatology at this point given the stance by the NRP so these sorts of studies I suspect will be the best we get.
For now, based on what is out there I suggest use the route that you can get first but expect to need additional doses at least one more time to achieve success. Lastly remember that even if you do everything correct there will be some that cannot be brought back. Rest assured though that if the first dose was given via ETT you have still done your best if that was the route you had.




 This study compared 5 different methods of delivering PPV to a 1 kg preterm manikin. The first was a standard self inflating bag, the next three different t-piece resuscitators and then the Next Step. For the first four the goal was to deliver a pressure of 20/5 at a rate of 40-60 breaths per minute. A test lung was connected to the manikin such that each device was used for a one minute period at three different levels of compliance (0.5 ml/cmH2O, 1.0 ml/cmH2O and then 2.0 ml/cm H2O representing increasing compliance. The goal of the study was to compare the methods in terms of delivering a volume of 5 mL to this 1 kg model lung. The order in which the devices were used was randomized for the 25 participants in the study who were all certified in NRP and included some Neonatologists.
This study compared 5 different methods of delivering PPV to a 1 kg preterm manikin. The first was a standard self inflating bag, the next three different t-piece resuscitators and then the Next Step. For the first four the goal was to deliver a pressure of 20/5 at a rate of 40-60 breaths per minute. A test lung was connected to the manikin such that each device was used for a one minute period at three different levels of compliance (0.5 ml/cmH2O, 1.0 ml/cmH2O and then 2.0 ml/cm H2O representing increasing compliance. The goal of the study was to compare the methods in terms of delivering a volume of 5 mL to this 1 kg model lung. The order in which the devices were used was randomized for the 25 participants in the study who were all certified in NRP and included some Neonatologists.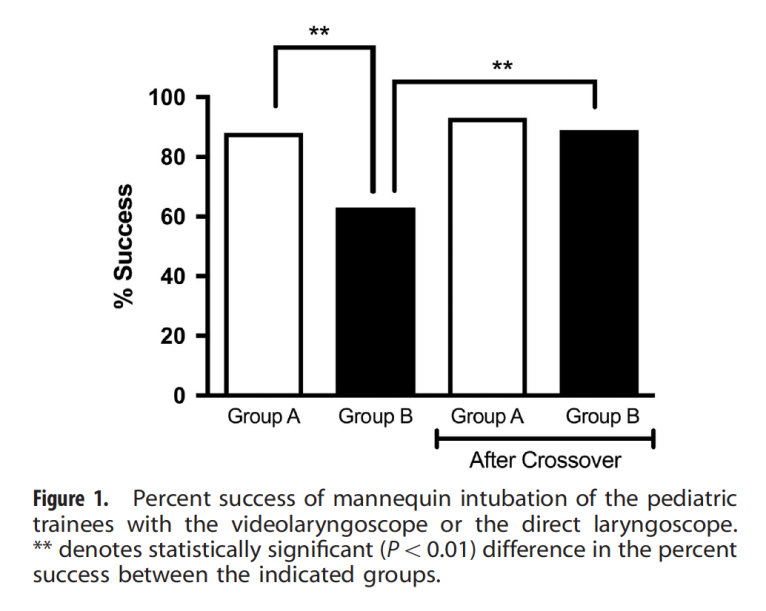 The findings demonstrated a couple interesting things. The first as shown in the graph was that the group that started with the laryngoscope had a near 90% success rate compared to about 60% for the traditional approach. When the groups swapped though they were both equal in effectiveness. This suggests that by visualizing the airway with the VL students were able to identify structures better after doing so such that success was improved simply by having used the device.
The findings demonstrated a couple interesting things. The first as shown in the graph was that the group that started with the laryngoscope had a near 90% success rate compared to about 60% for the traditional approach. When the groups swapped though they were both equal in effectiveness. This suggests that by visualizing the airway with the VL students were able to identify structures better after doing so such that success was improved simply by having used the device.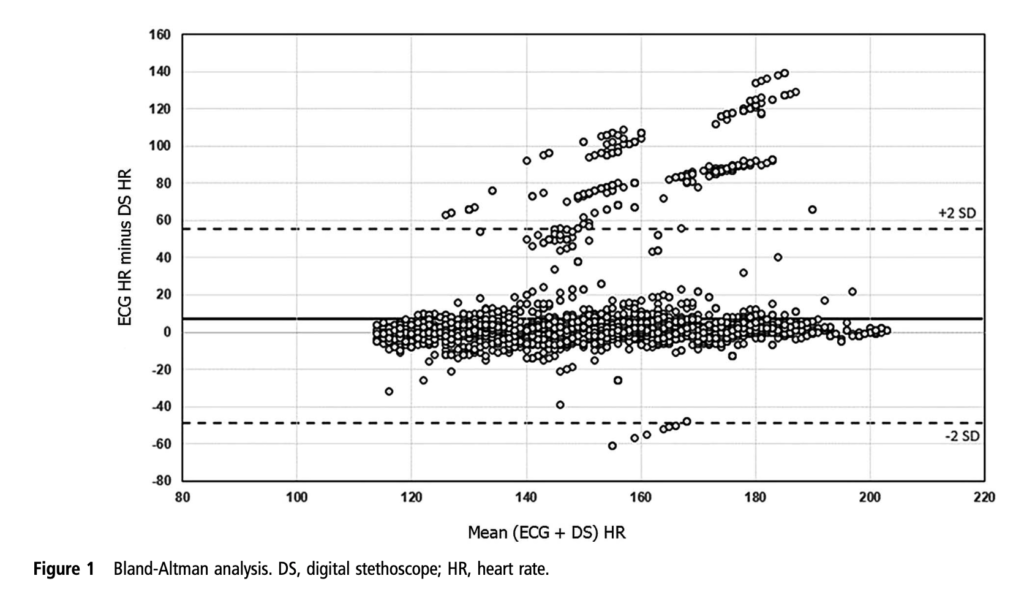 decided to look at the use of the Stethocloud to measure HR after birth in infants >26 weeks gestational age at birth. The opted to use the ECG leads as the gold standard which arguably is the most accurate method we have for detecting HR. The good news was that the time to signal acquisition was pretty impressive. The median time to first heart rate with the stethoscope was 2 secs (IQR 1-7 seconds). In comparison the time for a pulse oximeter to pick up HR is variable but may be as long as one minute. In low perfusion states it may be even longer or unable to pick up a good signal. The bad news was the accuracy as shown in the Bland Altman plot. The tendency of the stethoscope was to underestimate the EKG HR by about 7 BPM. Two standard deviations though had it underestimate by almost 60 BPM or overestimate by about 50 BPM. For the purposes of resuscitation, this range is far to great. The mean is acceptable but the precision around that mean is to wide. The other issue noted was the frequent missing data from loss of contact with the patient. Could you imagine for example having a baby who has a heart rate of 50 by the stethoscope but by EKG 100? Big difference in approach, especially if you didn’t have EKG leads on to confirm. The authors note that the accuracy is not sufficient and felt that an improvement in the software algorithms might help.
decided to look at the use of the Stethocloud to measure HR after birth in infants >26 weeks gestational age at birth. The opted to use the ECG leads as the gold standard which arguably is the most accurate method we have for detecting HR. The good news was that the time to signal acquisition was pretty impressive. The median time to first heart rate with the stethoscope was 2 secs (IQR 1-7 seconds). In comparison the time for a pulse oximeter to pick up HR is variable but may be as long as one minute. In low perfusion states it may be even longer or unable to pick up a good signal. The bad news was the accuracy as shown in the Bland Altman plot. The tendency of the stethoscope was to underestimate the EKG HR by about 7 BPM. Two standard deviations though had it underestimate by almost 60 BPM or overestimate by about 50 BPM. For the purposes of resuscitation, this range is far to great. The mean is acceptable but the precision around that mean is to wide. The other issue noted was the frequent missing data from loss of contact with the patient. Could you imagine for example having a baby who has a heart rate of 50 by the stethoscope but by EKG 100? Big difference in approach, especially if you didn’t have EKG leads on to confirm. The authors note that the accuracy is not sufficient and felt that an improvement in the software algorithms might help. There was virtually no difference between the ECG and the stethoscope with a 95% confidence interval as shown in the graphs with A being for all recordings and B being those without crying (which would interfere with the acquiring of HR). A maximal difference of +/- 18 BPM for all infants is better than what one gets with auscultation or palpation in terms of accuracy and let’s not forget the 2 second acquisition time!
There was virtually no difference between the ECG and the stethoscope with a 95% confidence interval as shown in the graphs with A being for all recordings and B being those without crying (which would interfere with the acquiring of HR). A maximal difference of +/- 18 BPM for all infants is better than what one gets with auscultation or palpation in terms of accuracy and let’s not forget the 2 second acquisition time!