

If you have a baby in the NICU there is a pretty good chance there will be at least one piece of plastic inserted into your child at some point. We have all sorts of “lines” and tubes that may be present depending on the conditions your baby develops. What follows is a primer on what they are all for.
IVs
I thought I would start with the easiest one since when you gave birth the team delivering you put one in you as well. The IV in the neonate is typically put in a hand or foot rather than the crease at the elbow as we like to save the bigger veins for something that we will talk about later on. Typically the IV provides sugar water (D10 most typically which is 10% sugar in water) to provide your baby with enough sugar to satisfy their metabolic needs. If a baby is older at birth but has difficulty breathing, having this type of access allows us to give them sugar and energy while not feeding them and letting their breathing settle. Putting food in the belly may sound like a necessity but they will be fine for awhile on dextrose which will allow their breathing to settle without having a full stomach pushing up on their diaphragm.
Umbilical Catheters
These come in two forms; the umbilical venous and arterial catheters. The easiest way to think of these are as long IVs like the one you may have had in your hand during delivery. These are long and on the venous side allow us to provide nutrition to your child either with sugar water (dextrose) or total parenteral nutrition (TPN). We can also give medications which can be tough on small veins in the hand or feet such as those to help with boosting blood pressure. The arterial catheter on the other hand allows us to monitor your baby’s blood pressure continuously. It also gives us a way of drawing blood when we need to test a number of things such as how your baby is breathing (an art gas) or checking their biochemistry such as when you hear us order “lytes” which checks salt and water balances in the body. By the way, putting these lines in does not hurt as there are no nerve endings in the umbilical cord.
Nasogastric Tubes
These plastic tubes go from the nose (or mouth if it is an orogastric tube) into the stomach. When your baby is too preterm to know how to suck, swallow and breathe without inhaling their food it is safest to provide their milk through one of these tubes. They are very common!
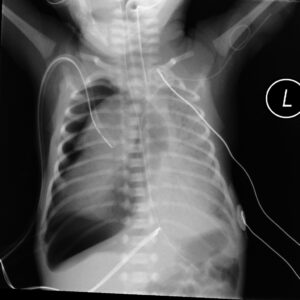
Endotracheal tubes
When your baby is unable to breathe on their own they may need to be put on a ventilator. The ventilator attaches to an endotracheal tube and helps your baby get oxygen in and carbon dioxide out. These tubes can also be used very briefly to administer surfactant which makes it easier for your baby’s lungs to open and take air in. You may hear the medical team refer to the INSURE approach when using the tube in this way which stands for Intubate, Surfactant, Extubate.
Chest Tubes
Thankfully these tubes are not needed as much as they used to be. When air gets in between the lung and the chest wall we call that a pneumothorax.
This air can build up and make it very difficult for the underlying lung to open and fill with air. When that happens your baby’s oxygen levels drop and the carbon dioxide rises. These tubes will be put in to drain the air and relieve the pressure. Once they stop “bubbling” the tube will be clamped and then pulled out if no air reaccumulates. You may also see these tubes placed when a baby develops fluid in the same space called a pleural effusion. In that case you are trying to get rid of the fluid rather than air that has found its way in between the lung and the chest wall.