

If you work in NICU you will have seen many babies who have passed through the stages of apnea, weaned off respiratory support and have reached a sufficient weight for discharge but alas will just not feed. Different strategies have been employed to get these infants feeding that rely in many cases on a cue based approach but in the end there are some that just won’t or can’t do it. Many of these babies will be sent home either with NG feedings or if it appears to be a more long term situation a gastrostomy tube. For this blog post I am going to present to you some novel research that suggests there may be another way to approach this and would like to thank one of the followers of my social media for alerting me to this work. You know who you are as the saying goes!
Transcutaneous Auricular Vagus Nerve Stimulation taVNS
This was an open label Phase 0 trial (few patients as a pilot) using taVNS to help improve feeding in ex-preterm or 3 recovering from HIE infants who were now past term and all headed towards a gastrostomy tube. The hospital carrying out the study entitled Transcutaneous Auricular Vagus Nerve Stimulation-Paired Rehabilitation for Oromotor Feeding Problems in Newborns: An Open-Label Pilot Study by Badran BW et al did not come out of thin air. Prior research in adult patients recovering from stroke found in multiple studies (all referenced in the paper) that motor stimulation accompanied by VNS improves motor function recovery. The objective here then was to see if stimulation of the auricular nerve along with assessment and motor treatments from an occupational therapist once a day could help improve feeding and avoid GT placement. The trial overview is as shown below.
The centre in which the study was done had a historical rate in this population of <10% of such patients avoiding a GT (all reaching term equivalent age and not showing an improvement in feeds). This was demonstrated in previous work by at the Medical University of South Carolina (MUSC). “Preterm infants who have not reached full PO feeds by 40-week gestational age (GA) and/or after 40 days of attempting PO feeds have a >90% chance of eventually needing G-tube implantation to achieve full enteral feeds (Ryan and Gehle, 2019).”
The Intervention
taVNS was done once a day during a bottle feed and timed with observed suckling and swallowing by an OT. The stimulation was stopped during a pause in feeding.
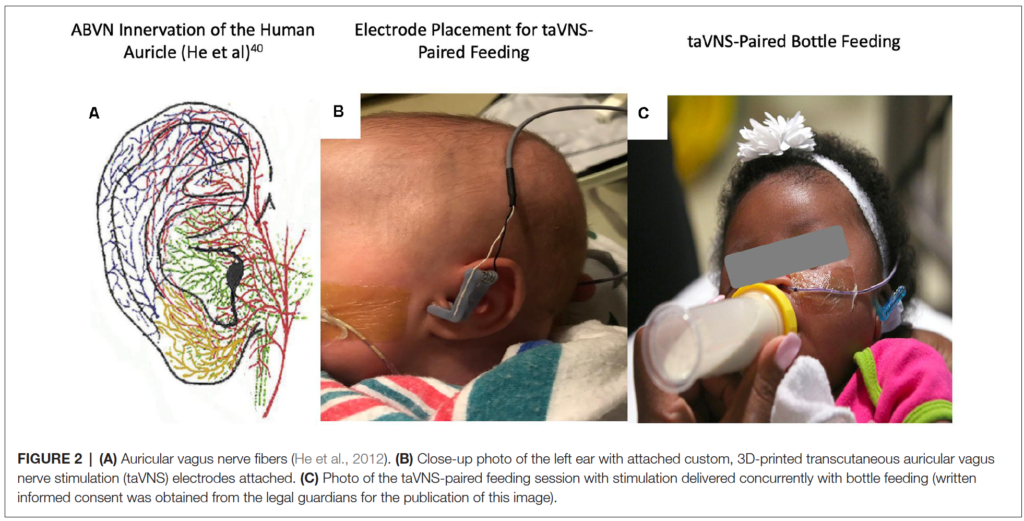
As you read this you may be concerned about side effects (as I was) of passing an electrical current to the ear and stimulating the auricular branch of the vagus nerve. This has been shown in other work to activate both afferent and efferent pathways of the vagus nerve and enhance plasticity and functional motor recovery. Could you then apply the same to improving development of the motor pathways of the preterm newborn or patient recovering from HIE? The authors examined skin irritation, pain scores and incidence of bradycardia before and during feeding while stimulation was occurring and found no difference in any of the measures. In order to minimize pain the authors increased the current by 0.1 mA until they perceived stimulation by change in facial expression, shrugging or fidgety movements. In the event of an increase in pain scoring by 3 the dose was decreased by the same amount. in the end the intervention was deemed safe without any adverse effects.
The primary outcome was ability to increase and maintain full daily PO intake for 4 days (>120 mL/kg/d and maintain a weight gain of >20 g/day until discharge.
Why you should care about the results
If you work in a hospital like mine you would probably find that once the discussion about a GT placement begins, few miraculously avoid it. In this study they found that 8 of the 14 patients or 57% avoided the GT. Their historical achievement in this regard was <10%. This could be by chance of course since the study is a small one but when looking at the PO intake between non-responders and responders they demonstrate the following.
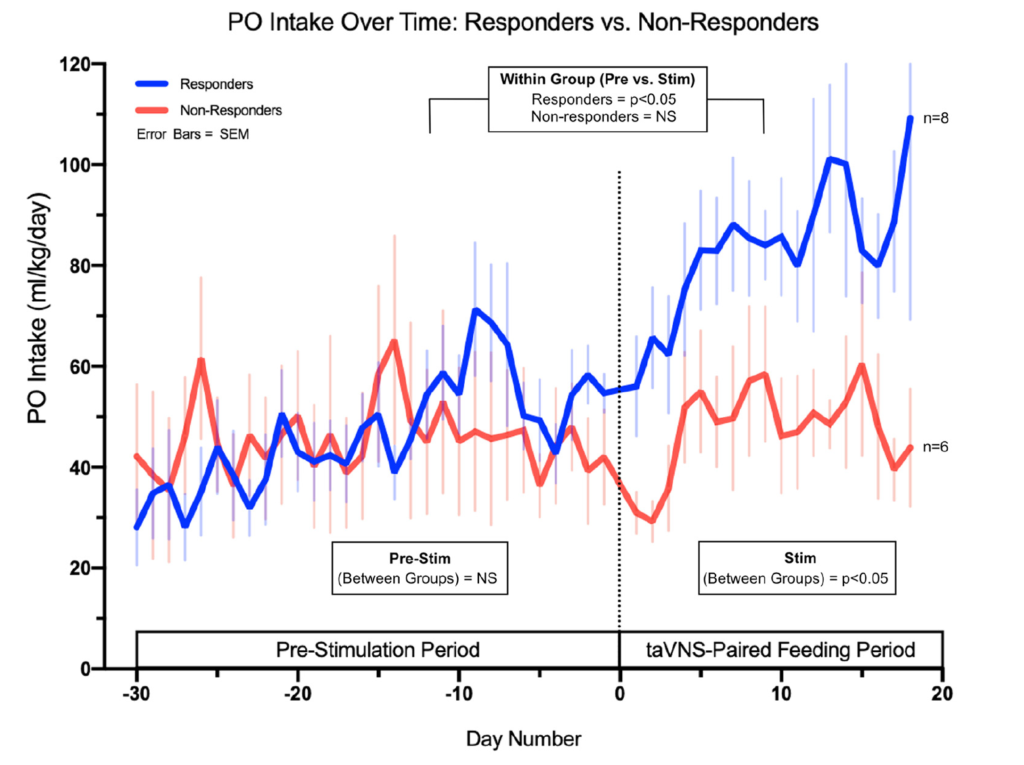
The authors found no statistically significant increase in the non-responders after the taVNS in PO feeds but also note there were three infants born to mothers with diabetes in this group. I have commented before on the effect of diabetes on successful feeding so this certainly could have affected the success of this group. If you look at the change over time in the responder group they look graphically like there was an upwards trend in the feeding ability prior to the intervention although the increase or slope of the improvement due to small numbers was not significant. The takeoff in feeding afterwards was.
The findings in this study are extremely exciting to me. As units across the globe struggle with patient flow, one of the most common reasons for these patients to stay in hospital is no longer BPD or apnea but inability to feed. The idea that such a simple intervention that is done once daily for 30 minutes might influence the development of feeding coordination in these at risk infants is phenomenal in terms of its impact on patient flow.
If you wonder about whether this is a one off study, there is a lot of active research in this area. A quick search of clinicaltrials.gov uncovers 61 studies on taVNS recruiting at the moment for a variety of ailments. In fact the next study is a Phase 1 trial aiming to recruit 40 patients and is underway. If interested the link to the study is here.
Stay tuned!