

Giving bronchodilators to preemies on a ventilator has certainly been tried before. The major issue to contend with is getting the drug to where it is supposed to be. Anyone reading who has a child with asthma knows that you should use an aerochamber when taking a puff to help with better distribution to the lung. Giving a puff or two without it largely ends up on the back of the throat. Similarly, giving puffs through an endotracheal tuberaises questions about how much of the medication winds up on the plastic tube rather than the smooth muscle of the airways where the medication is intended to be. This has been looked at in a cochrane review as well entitled Bronchodilators for the prevention and treatment of chronic lung disease in preterm infants
Can Albuterol Save The Day?
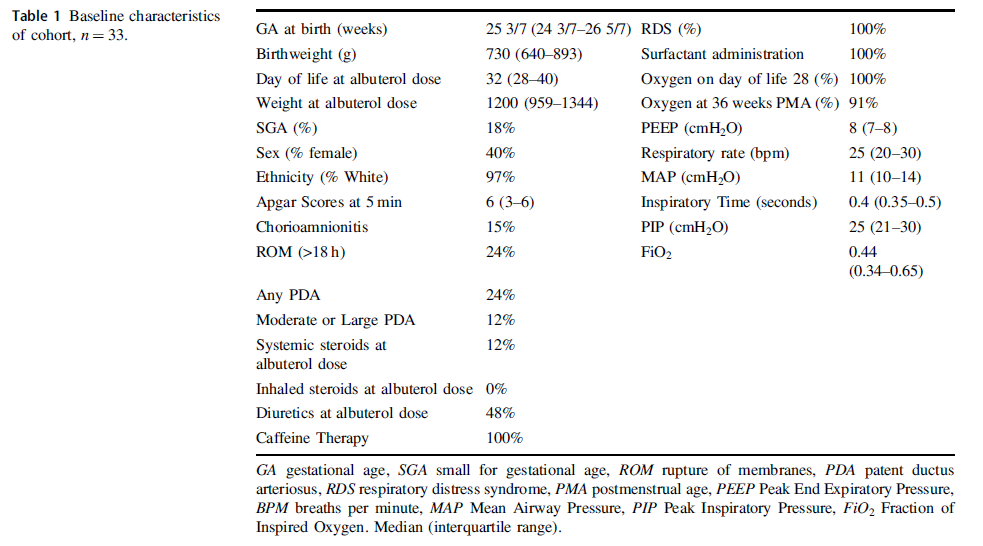
Albuterol is a beta agonist much like ventolin that can act on the smooth muscle of airways to achieve bronchodilation. Considering that preemies with immature lungs may have issues with both resistance and compliance, Raffay TM et al in their paper Response to first dose of inhaled albuterol in mechanically ventilated preterm infants chose to examine responsiveness in a group of 33 infants (all < 30 weeks at birth) to albuterol. Ideally, responsiveness would be done by pulmonary function testing but given that this was not possible in these infants they chose to examine other indicators of impact. After giving two puffs of 90 mcg of albeterol via a metered dose inhaler without an aerochamber the authors looked at changes in FiO2 as well as compliance and resistance measurements on the ventilator as a means of determining responsiveness. Ultimately, could they get drug into the distal airway in patients who were ventilated at about a month of age as shown in table 1 along with other baseline characteristics?
What makes this different than other studies I suppose is the use of the ventilator measurements and their use of histogram data on oxygen saturation to ascertain responsiveness to treatment. This was an observational study based on a secondary analysis of a previous study so we don’t have sham controls to compare to. Having said that by administering the medication and seeing what happens immediately afterwards it is possibile to get a sense of whether the drug had an effect.
So What if Any Effect Did It Have?
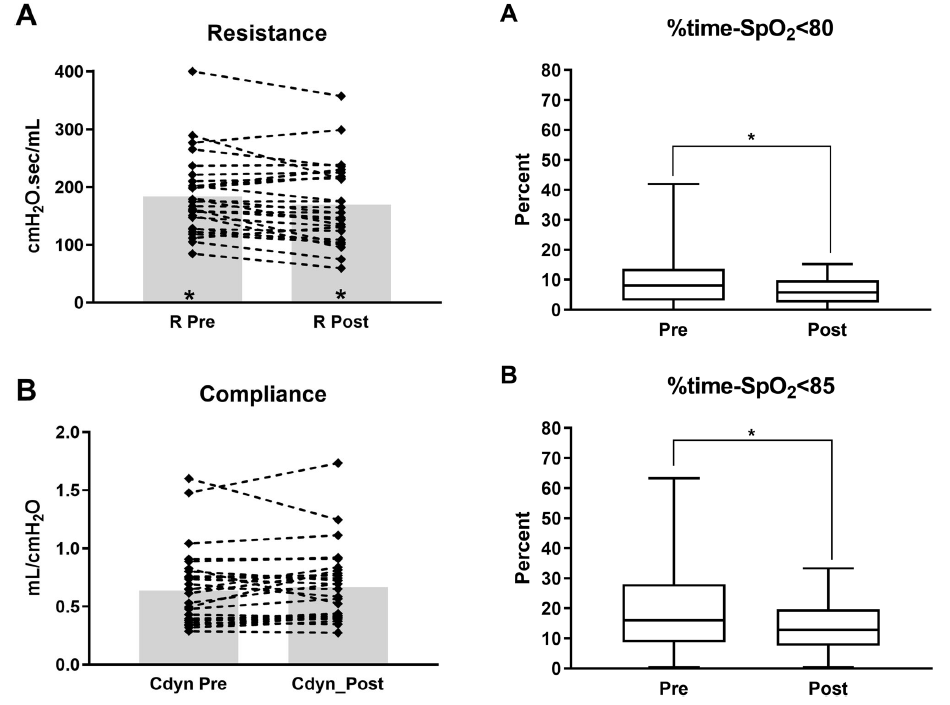
From the figure in the paper the answer is some effect. Overall, post albuterol resistance for the 33 patients overall was found to decrease. Compliance and FiO2 (not shown in the graphs below) did not change though. What did change however was the percentage of time spent below 80 and 85% respectively comparing a 4 hour window pre and a 4 hour window post with respect to histograms from the patient monitor.
Putting it together
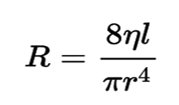
Ok so this isn’t a gold standard RCT looking at placebo treatments vs albuterol. It is hypothesis generating though as if resistance was decreased by albuterol one could expect improved delivery of O2 to the distal alveoli and therefore better oxygenation which is what is seen here. Should we be surprised that no difference in compliance is seen with albuterol therapy? I don’t think so as the effect of the drug is not on the distal alveoli and parenchyma but rather the more proximal branching airways. SInce airway resistance is governed by Poiseuille’s Law (you thought physics was over in high school?!) you can see that resistance (R) is directly proportional to the viscosity (n) and length (l) of the airway but inversely affected by the radius (r) to the 4th power. In other words if the radius of the airway after albuterol increases by 25% that effect is amplified to the 4th power in terms of reducing resistance.
I suppose I am buying what they are selling here but again the key is finding a method of getting the drug to deposit not in the trachea or proximal bronchi but to the lower airways. I can’t help but wonder if use of high frequency jet ventilation which carries flow down the centre of the airway might be a very effective way of getting such puffs further into the lung. Speculation of course but perhaps someone a little more creative than I can figure out how to do that and test deposition.
Should we use this routinely? Probably not as an everyday approach but it does make me wonder about those babies who are having a bad day so to speak. If one can glean from the ventilator that resistance has increased from one day to another might this be something worth trying? The authors found that the first treatment was effective but second and third not so much so to me this may just be a “hail mary” that is worth trying when nothing else seems to be working to reduce FiO2 in the presence of increased resistance.
If anyone is doing this routinely I would be curious in hearing your own experiences.