

It isn’t often that something comes along that causes me to raise not one but two eyebrows but I suppose the idea of adding insulin to preemies feeds is just such a thing. Apparently this research isn’t that new as there has been some previous animal research and human testing of breastmilk that revealed insulin is present in milk at concentrations of 46 microunit/mL. Testing of amniotic fluid has found even higher levels at 2500 microunits/mL! All of this insulin can’t be there by accident. If you believe in evolution as I do it can’t be by chance that all that insulin doesn’t have a role to play. By extension, since babies swallow amniotic fluid and therefore bath the developing intestine in insulin containing fluid there must be a benefit right?
Let’s do a study looking at benefits of oral insulin added to formula!
Researchers in Israel thought the same thing as they postulated that since insulin is a growth factor in the intestine that adding an oral formulation to formula may confer benefits. We know that breastmilk is better tolerated by preemies and might it be that the growth promoting effects of insulin in breastmilk is a contributing factor? There had already been a proof of concept Phase 1 study to test the use of oral insulin at 400 microunit/mL so on this go around the authors sought to perform a larger Phase 2 study looking at the primary outcome of time to full feeds. The paper is entitled Efficacy and Safety of Enteral Recombinant Human Insulin for Reduction of Time-to-Full Enteral Feeding inPreterm Infants: A Randomized, Double-blind, Placebo-Controlled Trial.
Infants included in this study were from 26-33 weeks GA with a birth weight greater than or equal to 750g and postnatal age < 7 days. Since breastmilk has insulin in it already all infants were fed formula. The insulin was NTRA as a dry powder with the dose of 400 microunit/mL chosen based on the amount known to be in amniotic fluid. The study required 76 patients but was stopped after 33 patients when a planned interim analysis found a benefit already to the intervention without any safety concerns identified.
The Results
The primary outcome was the time it took to reach full feedings defined as 150 mL/kg/d of enteral formula intake.
As you can see there was about a 1.6 day advantage favouring the group receiving insulin. This represents a 20% reduction in time to full feedings
In terms of secondary outcomes the results were also impressive even more so when one considers the small sample size. While we don’t routinely measure gastric residuals in our centre the authors did these measurements as a proxy for feeding tolerance. They defined low residuals as a goal of < 2 mL/kg in 24 hours. In the insulin group this goal was reached in 1.67 days vs 5.09 days in the placebo group. While this result had a p Value of 0.056 so therefore just missed being significant it is an interesting trend for sure. Again owing to small size while a difference in time to wean off TPN was 2.4 days shorter in the insulin group it was not significantly different. No difference it time to discharge was found but again the difference favoured the insulin group with a mean reduction of about 9 days for singletons.
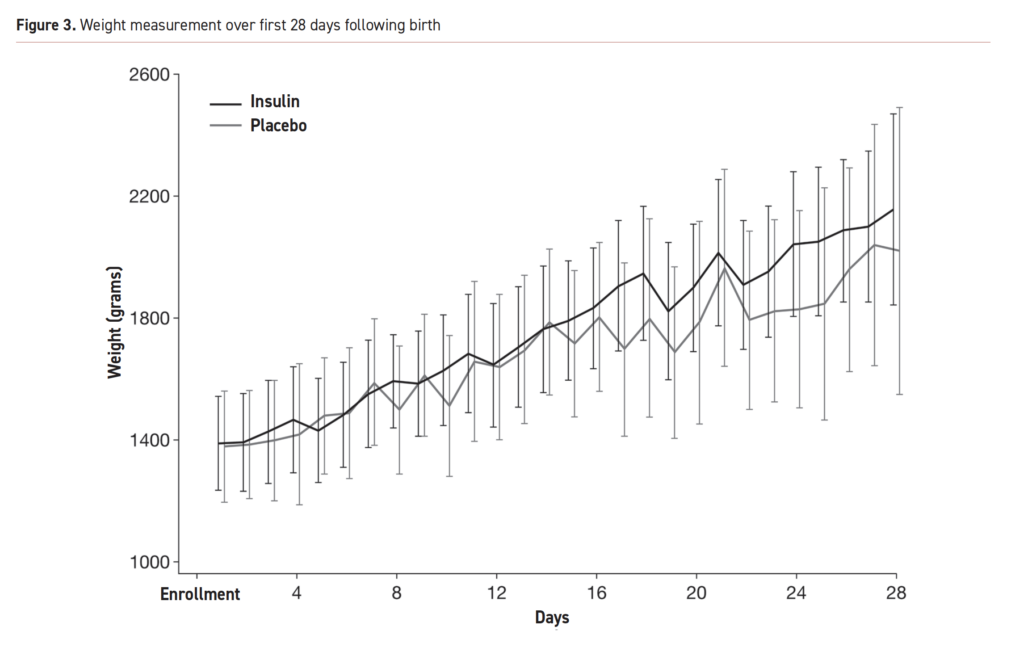
Below are the growth curves for the first 28 days reflecting a mean weight increase of 768.9g in the insulin group and 643.6g in the placebo arm.
So What’s Next?
I would like to start of by saying I hope one day you say you saw it here first! I think this research is very promising and no doubt a phase 3 trial with larger numbers is on the way. This isn’t quite ready for prime time as the saying goes based on small numbers but it is reassuring. Keep in mind this isn’t for everyone. We want as much as possible to provide breastmilk to our infants as it is more than just growth that we think about and time to full feeds. The question though for the future is whether for mothers who can’t produce enough or don’t want to breastfeed whether a little insulin sprinkled into their infant’s feeding will be just what the doctor ordered. My bet is that in the future you will see this indeed come into practice but we will need to certainly wait for bigger trials to confirm the trends that we are seeing here!@