

Skull fractures after birth. Don’t be so quick to blame.
Anyone who has watch the delivery of a baby knows that in some cases things go very smoothly and in others every care provider in the room would likely have tachycardia themselves. In some cases where labour is quite prolonged and some degree of cephalopelvic disproportion exists, the fetal head can become quite wedged in the pelvis. When this occurs it is not uncommon to hear of an ob/gyn having to dislodge the entrapped head from below and then perform a c-section to get the baby out safely.
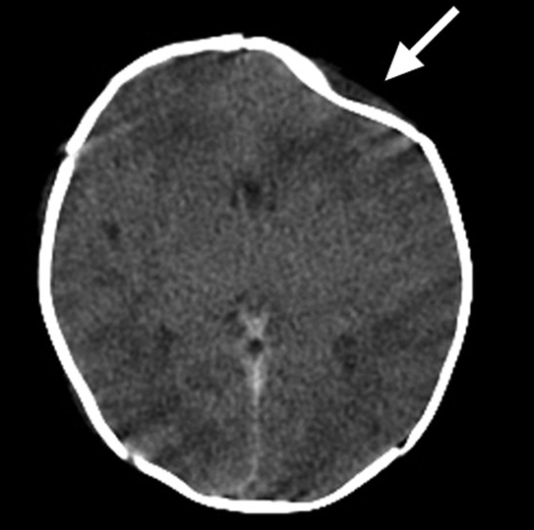
In some of these cases though on the newborn exam a depression of the skull is found such as with the figure on the right. As our brains like to link things together we may jump to the conclusion that the pressure exerted on the head from below led to a fracture. This fracture in turn may lead to injury to the underlying brain. At least that is what our brains want us to think but what if the reason for the fracture has nothing to do with the maneuver as described?
Spontaneous Skull Fractures
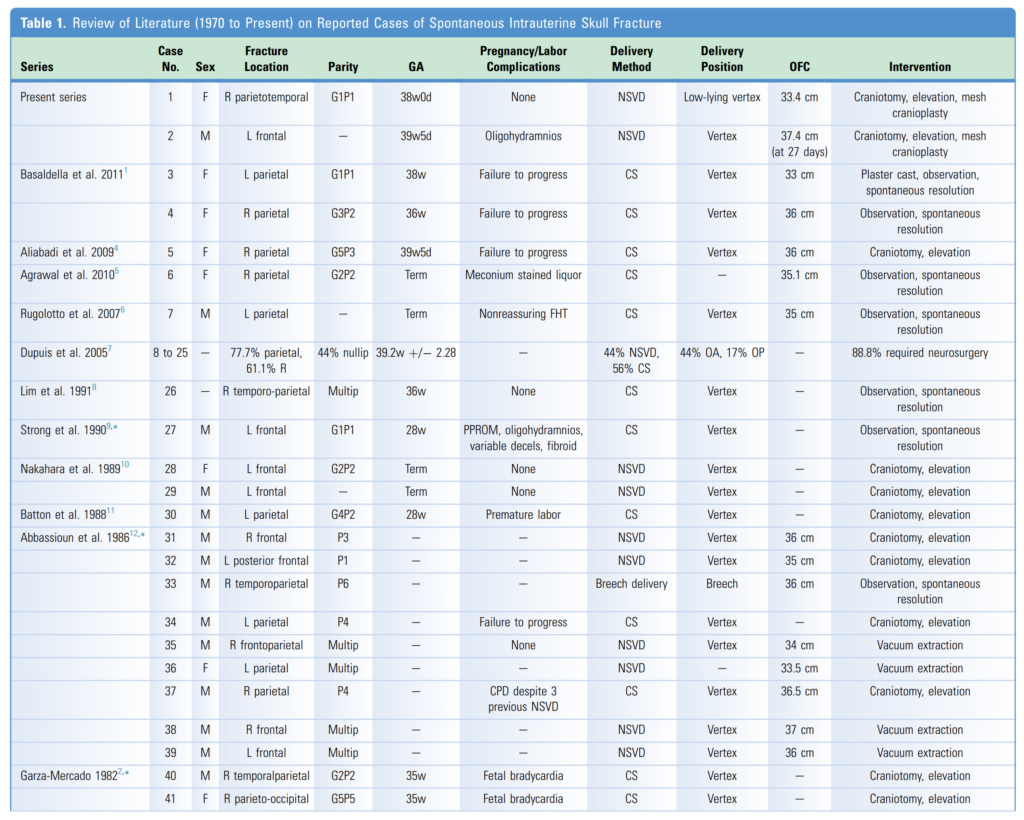
This exact situation has been described in two cases and with a review of the literature in a paper entitled Spontaneous Intrauterine Depressed Skull Fractures: Report of 2 Cases Requiring Neurosurgical Intervention and Literature Review. In this report they describe two cases, the first of which was a term infant born via SVD without instrumentation and was described as atraumatic. The figure above was from this infant and thankfully the underlying brain was free of hemorrhage. The second case was also term and again there was no need for forceps or vacuum. In this case there was significant parietal fracture with a small amount of subdural blood collection. This infant unlike the other one due to significant depression required neurosurgical intervention to correct the skull deformity and lift the bone off the brain. As the authors go on to describe there have been 39 other such patients described in the literature with the features as shown in the table from the paper. While there are 4 more in the paper they had vacuum extractions so I wouldn’t count them.
Why Does This Happen?
The short answer in most cases is a tight fit! In the 1960s this was postulated that in the right occiput posterior and and right occiput transverse positions the fetal head becomes compressed between the sacral promontory and pubic bones. Other implicating factors have been maternal fibroids leading to chronic pressure on the developing skull along with oligohydramnios that may lead to fetal compression as well.
When you look at the above table though what stands out is failure to progress as an ethology. One can imagine the contracting uterus attempting to propel the fetus forward and if impacted in the pelvis the pressure on the skull may well lead to fracture.
The other thing of note is the overwhelming involvement of the parietal bone in these cases. A presentation in another bone might lead one to think of a different etiology.
As far as treatment, many of these as you can see are simply observed but in the presence of significant bleeding neurosurgical intervention is needed. At the outset it is sensible to consult neurosurgery as one never knows which ones need intervention and which ones do not.
As you can see, the presence of a fracture and a history of forceful pushing from below MAY be related to a fracture but on the other hand these may occur simply with protracted labours themselves. In these situations while it may be tempting to blame the ob/gyn we also need to ask ourselves what the alternative they had was. Should they have let the mother continue to push with the potential risk of asphyxia or potentially even uterine rupture? At some point the delivering physician needs to get the baby out and if that is what needs to be done to extract the baby then that is what they will need to do. At the end of the day one thing is for sure that we don’t know for sure what caused the fracture and as tempting as it may be to blame the ob/gyn or GP delivering a baby it just might have been spontaneous!