I recently had the honour of being asked to present grand rounds at the University of Manitoba. My former Department Head during the question period stumped me when he asked me what role angiotensin converting enzyme 2 receptor (ACE2) has in pediatric COVID19. Like all great teachers, after I floundered and had to confess that while I was aware there is a role in COVID19 I wasn’t sure of the answer, he sent me a paper on the subject. The reality is that a very small percentage of COVID19 illness is found in children. Some estimates have it at 2%. Why might that be?
It’s what’s in the nose that matters
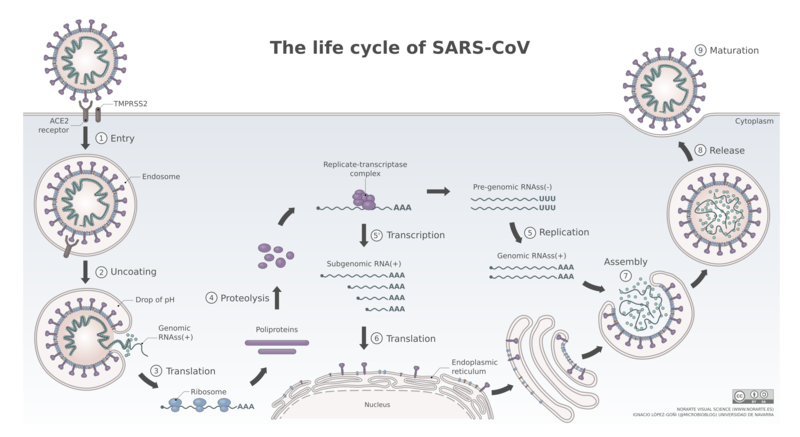
What has been known for some time know is that the point of entry for SARS-CoV-2 is the nasal epithelium. What is also known is that the receptor that the virus binds to in order to gain access to the host. Such binding and what happens after the virus gains entry to the body is shown in this figure depicting the life cycle of SARS-CoV-2.
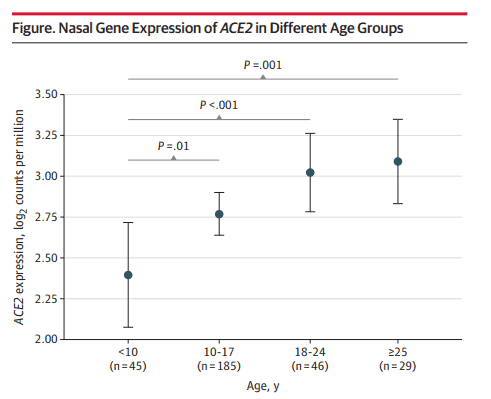
In a research letter by Bunyavanich et al Nasal Gene Expression of Angiotensin-Converting Enzyme 2 in Children and Adults looked at 305 patients from ages 4-60 years to examine biomarkers of asthma. In the course of looking at the nasal epithelium of these patients, they found age related differences in the expression of ACE2 receptors as shown in the following figure.
I think the results somewhat speak for themselves. The younger you are the less receptors you have. If you have less receptors maybe you are less likely to contract the virus!
What we don’t know
This research leads to some interesting questions. Drugs such as losartan and valsartan already exist and function by blocking he ACE2 receptor. Could blockade help to limit the spread of infection? I am not aware of any such trials going on at the moment but something worth looking at.
The other point that needs to be raised is that the most vulnerable group of ages >60 were not looked at in this study. The trend would certainly indicate that with age we would expect the receptor numbers to increase but since we don’t actually have the data in the older groups we don’t know if receptor numbers start to fall again with age. Similarly we don’t know below the age of 4 what receptor numbers are like. In examining risk of vertical transmission it is worth noting that the recent placental positive RT-PCRs as in Detection of SARS-COV-2 in Placental and Fetal Membrane Samples. In that study while 3 of 11 placental membranes tested positive, none of the newborns were infected. Could it be the fetus and newborn is protected by having very little density of ACE2 receptors? Something to look at and will be no doubt.
Regardless, in the fight against COVID19 maybe one direction for therapeutic targeting should be addressing this receptor and seeing if there is something we can’t do to make it less susceptible to binding.
For more Neonatal subjects be sure to see my Facebook page at https://www.facebook.com/allthingsneonatal2
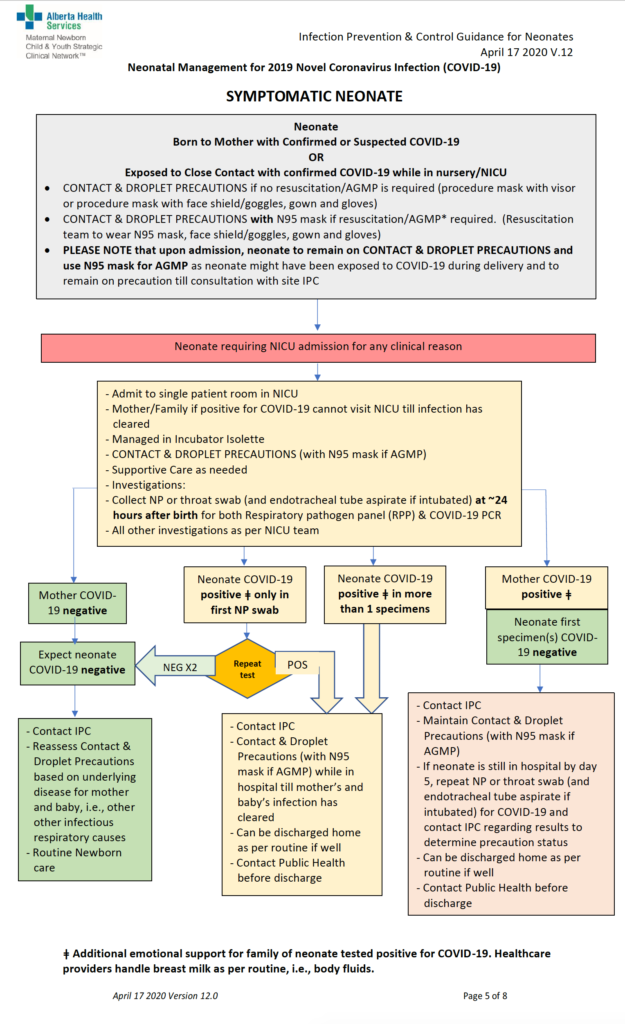
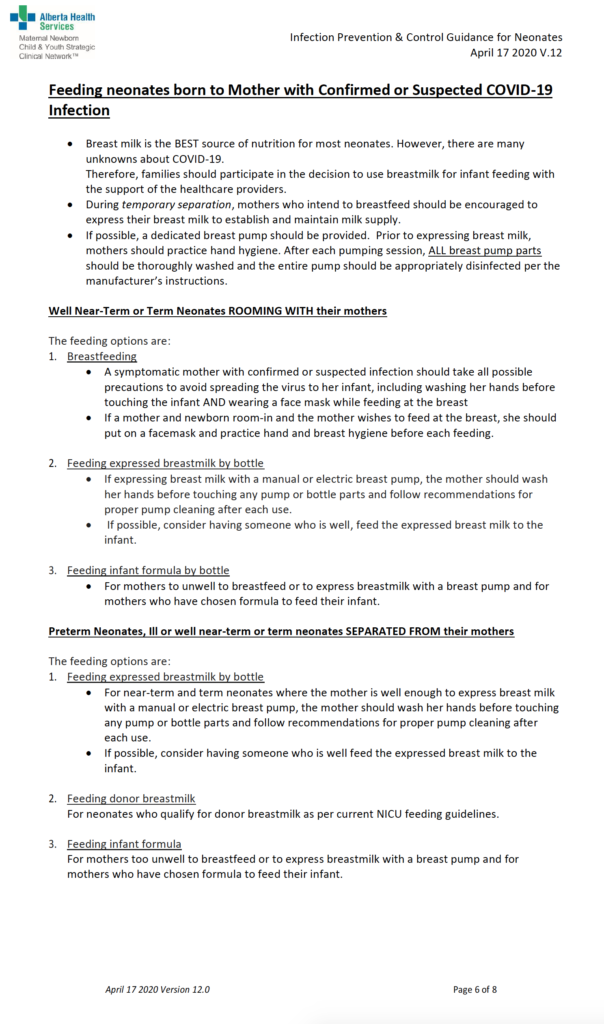
After several reports providing reassurance to breastfeeding mothers, two very recent reports are giving me reason to pause. The Canadian Pediatric Society has been recommending breastfeeding if a mother has COVID19 with precautions in place; Breastfeeding when mothers have suspected or proven COVID-19. It would be heresy to suggest that a mother not be permitted to breastfeed her infant but what follows are two reports that at the very least may need to enter the discussion when a COVID19 positive mother gives birth and is deciding about route of feeding.
Toronto Case Report
The first report was notable not so much for breastmilk but rather that a mother with a chronic immunodeficiency and pneumonia from COVID19 had placental surfaces that tested positive on PCR for COVID19. This was the main focus of the paper Probable congenital SARS-CoV-2 infection in a neonate born to a woman with active SARS-CoV-2 infection. In the same paper though, testing of breastmilk in this mother demonstrated a positive PCR with a semi-quantitative cycle time result (there are 40 cycles of amplification of RNA in PCR testing- the further away from 40 cycles the more likely it is a true positive).
The results above were positive at 2 days and negative at 7 days. One could possibly excuse this case as an anomaly since the mother in this case not only was sick but also has chronic neutropenia but then along comes another report.
Second Research Report
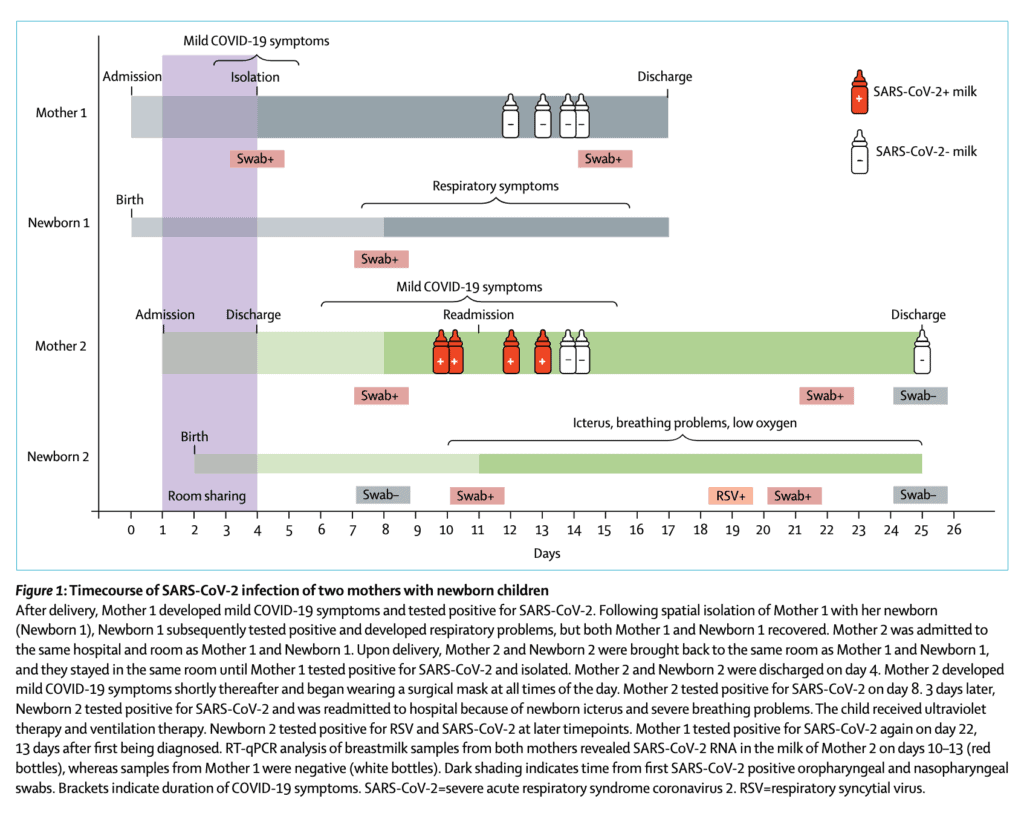
This week a second report emerged that adds to the uncertainty around breastmilk. Detection of SARS-CoV-2 in human breastmilk looks at two mothers one of whom was negative on testing of breastmilk but the other unfortunately tested positive. The authors included the following timeline which is very informative.
From the timeline above you will note that in the second case the mother becomes positive at 11 days of age and the infant tests positive around the same time the milk comes back positive. The infant in this case also develops RSV which likely explains the symptoms they developed later in the course. What is concerning to me though is that in this case while the mother was COVID19 positive, she was not acutely ill. When thinking of vertical transmission this has been something that has been postulated in suspecting that those with more severe illness have higher viral loads and therefore may be capable of vertical transmission. Not the case here if the results are to be believed. Adding to the strength of the result are Ct values for SARSCoV2 N peaked at 29∙8 and 30∙4 in whole milk and skimmed milk respectively so this seems real.
How does this differ than past testing?
What intrigues me about this study in particular is that past research on transmission into breastmilk has failed to detect the virus. It could be that previous testing close to delivery was negative and that with time might the virus enter breastmilk? At eleven days I think this may be the latest testing done. In virtually all cases reported about COVID19 positives in newborns the authors have always explained the painstaking steps they took to prevent postnatal infection. I do wonder now if some of these cases may be related to a small percentage of women carrying the virus in their breastmilk. This leaves us in a tough spot. What do we tell women who are thinking of breastfeeding and have COVID19? There will need to be discussion on this but one option is to proceed with feeding accepting there may be a small risk of transmission. A second option would be to test milk but if the transmission occurs late you may miss it in hospital on initial sampling Finally it may be worth pumping and discarding milk until mothers test negative and using donor breastmilk in the meantime (or formula for those who don’t have DBM).
Regardless I think this information coming out will need to be digested and centres think about how they will approach this issue. My guess is these will not be the last reports on this.
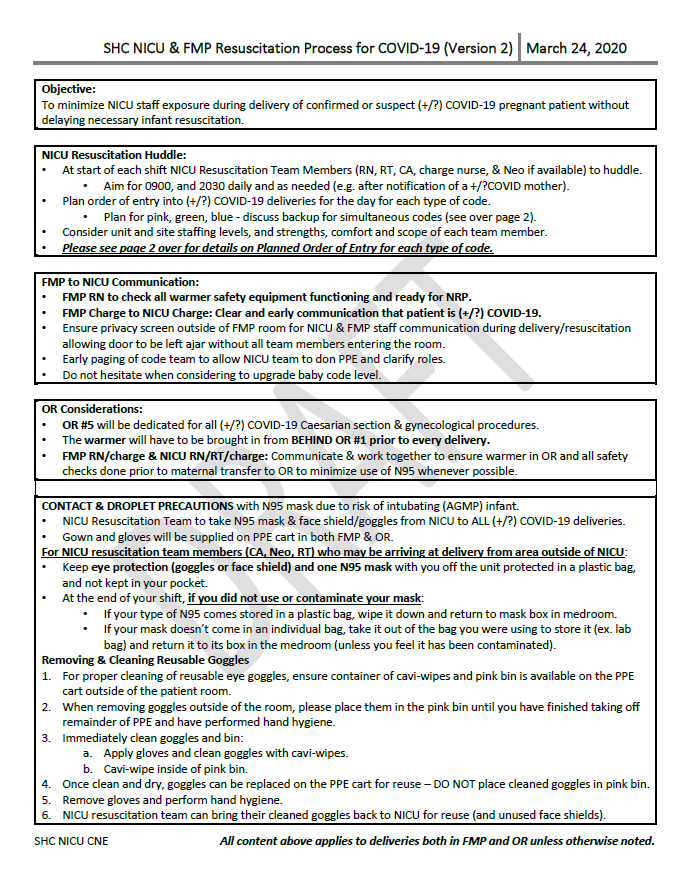
I had the pleasure of being asked to speak to a Canadian audience of people working with newborns yesterday about the new CPS practice points for managing deliveries and newborns with suspected or proven COVID-19. Something fascinating happened over the course of the discussion and that was that we are a country divided. It didn’t help that the week prior to the CPS releasing their practice points the American Academy of Pediatrics released the following position:
“Precautions for birth attendants: Staff attending a birth when the mother has COVID-19 should use gown and gloves, with either an N95 respiratory mask and eye protection goggles or with an air-purifying respirator that provides eye protection. The protection is needed due to the likelihood of maternal virus aerosols and the potential need to perform newborn resuscitation that can generate aerosols.”
I don’t know how the Americans are going to deliver on bringing N95 masks to all deliveries and even acknowledge in their statement that this recommendation essentially holds as long as there are supplies. There are a lot of deliveries in the US and if every one requires all team members to have an N95 respirator (two nurses, RRT, MD) that will burn through supplies quickly!
The driver of this division in the country and the AAP I believe is fear butI am not in any way judging anyone for having it in these trying times. I think it is worth looking at what is being proposed for care of the newborn by the CPS and what may be motivating this fear. Who knows it may help someone work through their own feelings on this.
What has been recommended?
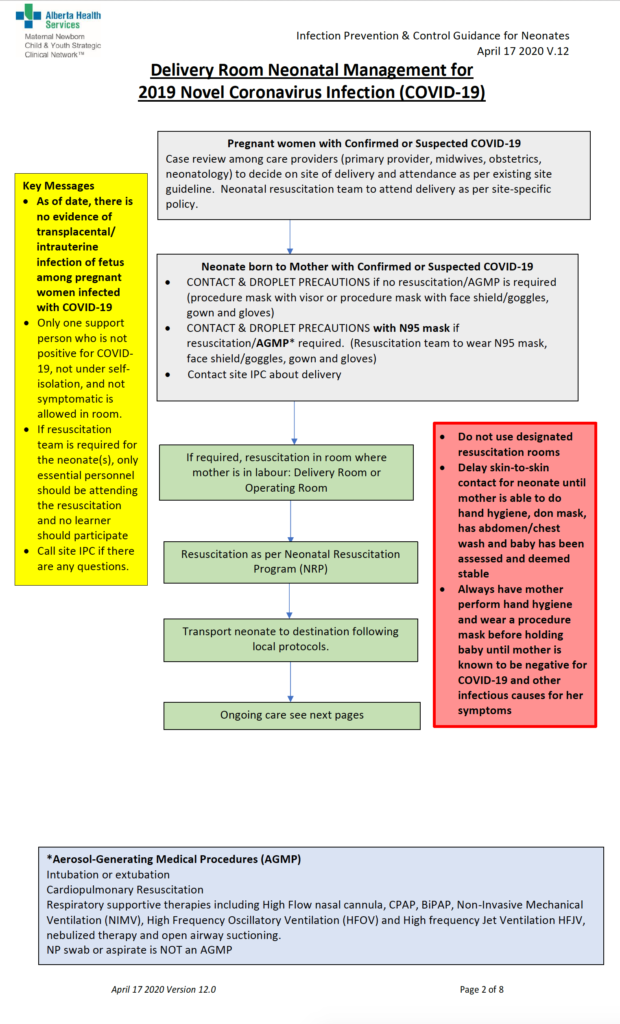
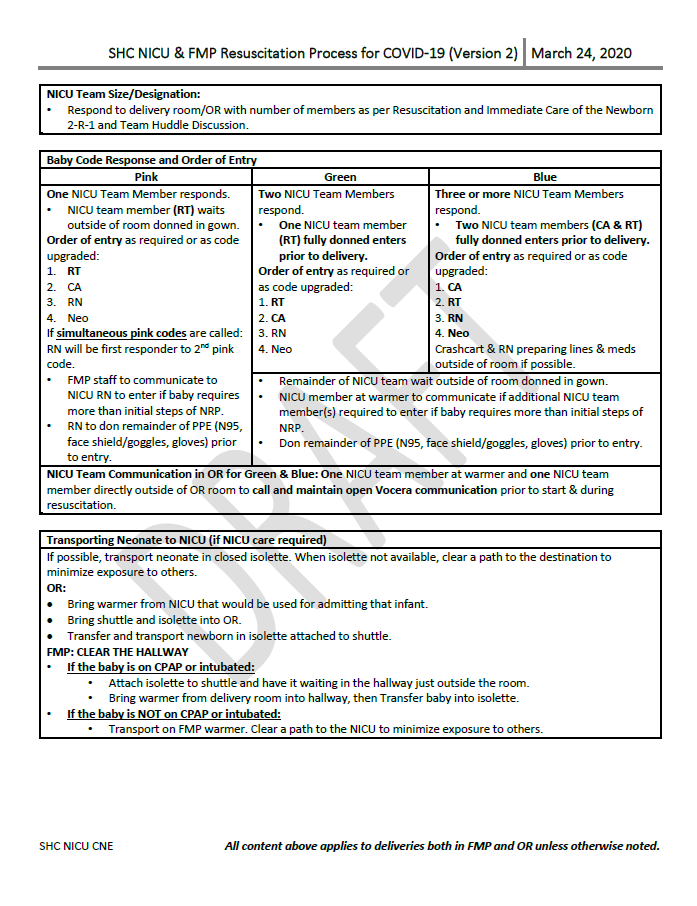
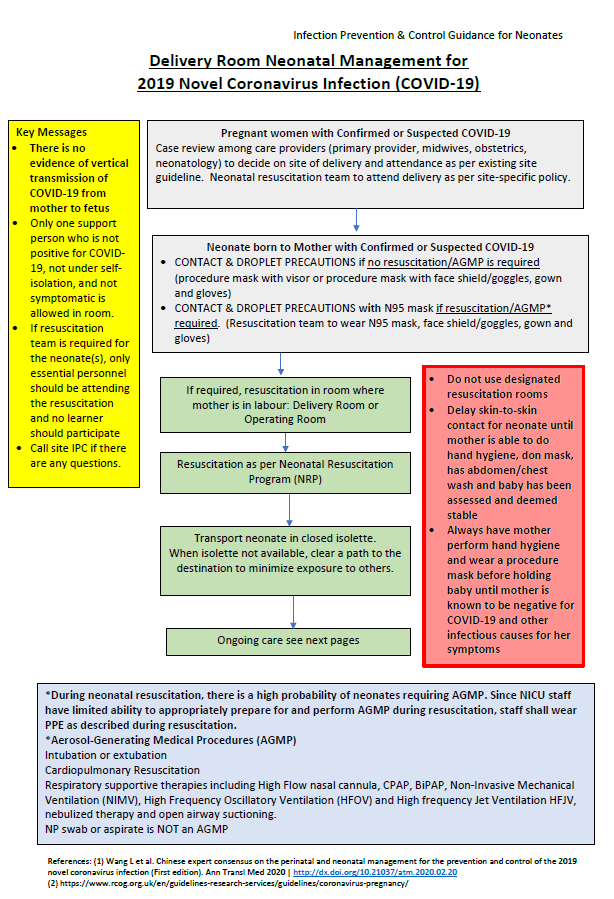
What the CPS recommendations boil down to is this. For attendance at a delivery in which the mother is not intubated or expected to be, providers of care for the newborn should use droplet precautions. Specifically, whether the infant is going to receive PPV, CPAP or be intubated the evidence strongly suggests the newborn is delivered uninfected so an N95 is not needed to protect health care providers. Even if the baby is born vaginally and is exposed to blood and stool, the viral load in the distal tracheobronchial tree will be low to non-existent so aerosolization would not be a concern. If the mother is going to be intubated then an N95 mask should be worn instead of a surgical mask. Outside of the delivery room in the NICU one should use an N95 mask for providing care to any newborns on CPAP or other non-invasive support as well as those who are intubated.
It is the last statement that I know has caused some confusion. Why is it that Dr. Narvey is suggesting that in the first 30 minutes of resuscitation we don’t need an N95 but then after the baby is moved to NICU we do? The issue is a pragmatic one. The earliest known case of a positive nasopharyngeal swab is 36 hours. This doesn’t mean of course that the earliest one can get horizontal transmission is 36 hours as this is when the health care providers decided to test. Presumably they were not lucky and timed it right so we have to expect at some point maybe hours or more earlier the baby became infected. As we get busier with more and more COVID suspect mothers there is a risk of people not “watching the clock” and therefore if we had said once 12 hours or 24 hours have elapsed use N95 masks for those on respiratory support we run the risk of someone losing track of time. There are a lot of babies who need PPV at birth though but not all eventually need CPAP so eliminating the need to use N95 masks when the evidence doesn’t support their use is a responsible way of preserving masks that are in short supply for those who truly need them based on true proven risk such as with adults with COVID pneumonia being intubated.
Why is there so much fear?
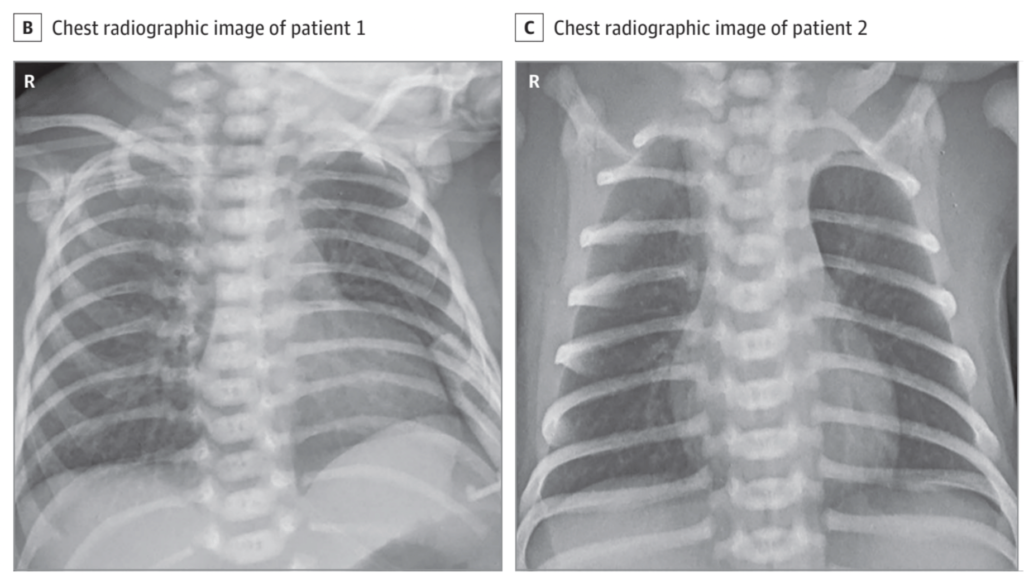
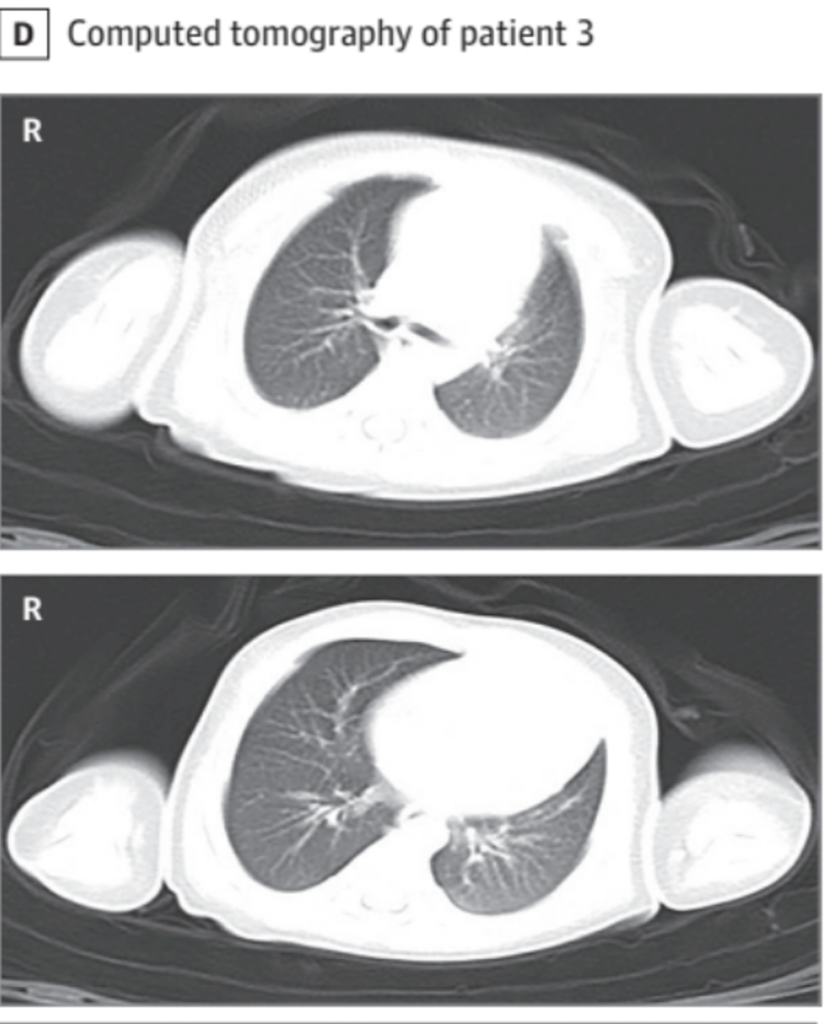
I blame the media to a great extent. They latch on to stories such as this one that made its way around twitter and facebook and yet there are no publications of this infant. Likely a positive infant no doubt but I suspect it was not detected minutes after birth. Then there is the case series in Jama Pediatrics that turned the world upside down a few weeks ago. I don’t know about you but my inbox was peppered with this paper from all over Canada and beyond. Looking at the paper in detail including the images is informative as what was initially touted as evidence of vertical transmission on closer inspection I think is far from it. Three out of thirty three infants tested positive on an NPA at 48 hours of age with a claim that all three had pneumonia. The authors included two x-rays for the two 40 week infants and a CT scan of the chest for the 31 week infant. Take a look at these films.
I am not a radiologist but I suspect we would have reported these films as normal. The CT scan of the chest is in a 31 week infant who had RDS and enterobacter sepsis. How would one differentiate RDS, enterobacter pneumonia or COVID19? It may be possible these three babies indeed were inoculated in the first day or two with COVID19 but I am not so sure they really had disease. If you agree with my argument here then we have multiple case series demonstrating no vertical transmission and this one case series indicating possible horizontal transmission. Why then are we hearing about care providers bring N95 masks to deliveries just in case CPAP is needed?
Fear is a great motivator
It likely comes down to the “what if” argument. What if everyone is wrong and babies can be born with COVID19? If we had an unlimited supply of N95 masks then my answer to everyone would be “if it makes you feel better then go for it and use away”. My argument for not using them at birth is twofold. Firstly, the evidence so far is that this is not a risk and secondly we don’t have an unlimited supply of N95 masks. This creates an issue for society as a whole that if we are guided by our fear we may deprive those who truly need this resource for evidence supported high risk procedures. I believe we all have a duty to provide the best care possible and working within a system with a finite amount of resources we need to really consider what happens if we let fear override what we know from evidence.
Having said all that (and this is not a cop out but reality), we are all fatigued and probably not at our best at the moment. We are fearful for our own heath and not just physicial but mental as well. I read this morning that suicide rates in the US are up 35% this year and extrapolating I would imagine that rates of depression and anxiety have gone up with it. These infants we care for deserve us to be at our very best. If fear of contracting COVID19 has reached a level for an individual that it may interfere with their ability to provide the proper steps of NRP if not wearing their “armor” in the form of an N95 mask this needs to be considered. I am not a psychiatrist nor am I pretending to be one but our mental state has a great impact on performance. I am not endorsing the use of N95 masks for everyone but I am suggesting that during this time we all take a moment and do a check in with yourself. Are you focused, are you able to think with a clear head when needed? We need to be at our best and for me I am confident that I can care for a newborn with a regular mask but I ask you since you know yourself to be truthful with yourself so we can provide the best care possible.
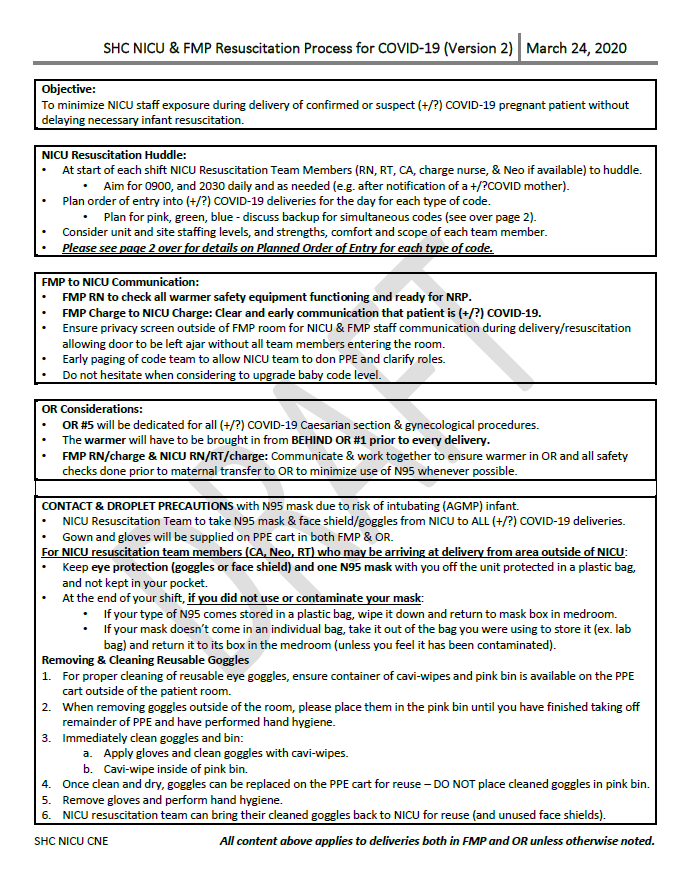
Things are tough out there. If you are pregnant you no doubt have lots of questions about living and ultimately giving birth during this difficult time. These guidelines are from Alberta and like with everything these days are subject to change. As of March 23, 2020 this is what is being recommended if you live in Alberta. There are many good things here that are universal no matter where you live. Social distance, wash your hands, avoid touching your face and stay at home if possible.