In NICU we are always vigilant for infections. Bacterial sepsis is not uncommon and in fact in the latest 2020 Canadian Neonatal Network annual report, 9.4% of all babies across Canada born at < 33 weeks gestation experienced an infection after 3 days of age. Looking at the rate of infections in those with central lines (Central Line Bloodstream Infection or CLABSI the rate was 2.9/1000 line days. Infections in NICU are not surprising given that these infants often have need for vascular access and needle pokes breaking the skin and have a somewhat fragile immune system associated with premature birth. There are many strategies to reduce infection risk in the NICU but one in particular that has been around a long time is cleansing of the skin before any skin breaking procedures are performed such as for blood draws. Options exist for cleaning in terms of solution and whether it contains alcohol or not. A common skin antiseptic used is chlorhexidine which comes available as a 2% or 1% solution and with or without alcohol. The babies in particular who are our smallest may be sensitive to the alcohol and may be left with skin burns so for the smallest of infants we often clean without the alcohol containing solutions. What we are going to talk about today though is the use of 2% vs 1% and whether one is any different than the other in terms of effectiveness.
The Study
The study was done in India by Sharma A et al and entitled Aqueous chlorhexidine 1% versus 2% for neonatal skin antisepsis: a randomised non-inferiority trial. The authors set out to determine a number of things. The primary outcome was the percentage of negative skin swabs after application of both but they also looked for evidence of harm in terms of skin rashes and chlorhexidine blood levels. The strategy employed was for the investigator to identify a 4cm2 skin area to obtain the pre-antisepsis skin swab from one of the following sites: cubital fossa, dorsum hand or dorsum foot. Each patient could be enrolled again after a 96 hour period of time had elapsed. An alternate site was selected at the time of repeat enrolment. Each patient had a swab of this area done in a specific and repeated way in terms of strokes of the skin and then in a randomized fashion each patient received either the 1% or 2% solution on a swab. The solution was tested by a pharmacist throughout the study to validate the concentration of chlorhexidine (swab was dipped in the tested solution) and then applied in a consistent manner to the skin area. The area was left to dry for 60 seconds and then a second swab taken to determine whether the skin had been cleared of the bacteria that would have been picked up by the swab pre-chlorhexidine. The study set a target of a 5% non-inferiority limit comparing the two concentrations with an expected efficacy of about 90% for a 2% chlorhexidine solution to sterilize an area. This meant that if the efficacy of the 1% solution fell below a 5% difference it would be deemed to not be equivalent to the 2%.
What did they find?
First of all the groups were comparable in baseline characteristics. The babies enrolled in the study ranged from 26 0/7 to 42 6/7 weeks at delivery. As planned the groups; 341 to 1% and 344 to 2% were stratified for analysis into 26 0/7 to 27 6/7, 28 0/7 to 34 6/7 and 35 0/7 to 42 6/7 groups. The means GA and BW for each overall group however were 2018 vs 2029 and 34 vs 35 weeks for 1 and 2% groups.
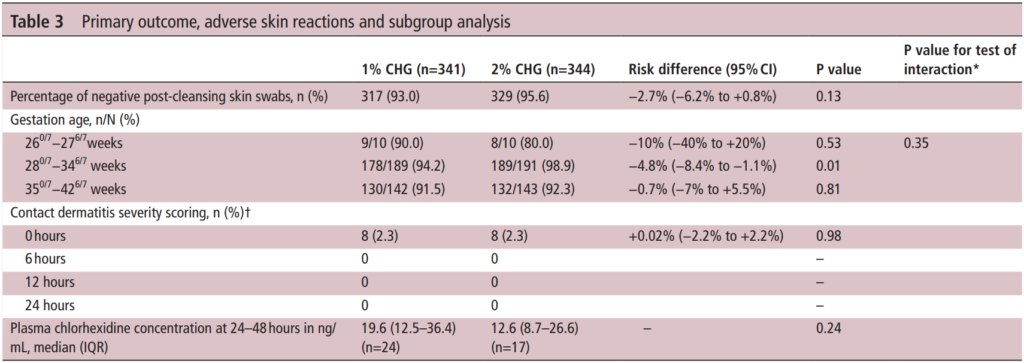
The table above has all the relevant information from the outcomes of interest. The efficacy of the antiseptics was a bit better than anticipated at 93% for the 1% vs 95.6% for the 2% group. On the surface you might be tempted to jump up and say “ah ha! They are equal”. However when you look at the 95% CI around the estimates you get a risk difference of -2.7% but the lower CI limit is -6.2% so as the authors concluded they are in fact not equal. Looking at the subgroups the number show some differences but only the middle group reached a statistical difference.
Importantly contact dermatitis which was scored by nursing using a standardized approach showed no difference at any time points. As expected some absorption did occur from application of the swabs but there was no difference between the two concentrations of significance although interestingly the higher concentration solution trended lower.
The authors do point out in this study that they did not get the 355 patients they wanted in each group although I have to say it was so close that I don’t believe adding a small percentage more of patients to the study would have been likely to change the conclusions.
Lesson from this study?
I suppose the first thing I take is that I am relieved that since our unit uses the 2% solution I don’t see any need for change. The second thing is that the rate of dermatitis from either solution is limited to about 1/10 babies after application but by 6 hours it is gone. Both have very high rates of successful skin antisepsis but if there is really no contraindication in terms of either skin irritation or high levels of drug in the blood my bias would be to grab onto the extra few percent successes at clearing the skin of bacteria. Even if it only a 3% gain, if we can maximize the cleaning of the skin before we poke a needle through it I think that is the way to go. If there are centres out there using the 1% though and plan on sticking to it I would be curious as to why?
This post is a written as a tribute to John Minski RRT who taught me much about ventilation over the years and has been a champion for innovation in our unit. As he prepares to move on to the next phase of his life I thought it would be a nice send off to talk about something that he has been passionate about for some time. That passion is inhaled nitric oxide for more than just pulmonary hypertension.
Prior Evidence
This is actually nothing really new. For a review on the background behind the theory you can read The potential of nitric oxide releasing therapies as antimicrobial agents. While we think of iNO as being a drug for pulmonary hypertension it has other capabilities. It can diffuse across cell membranes and damage pathogens by causing nitrosative and oxidative damage. The amount of iNO needed though to accomplish this bactericidal action is much higher than the typical levels of 20 – 40 ppm that we use. Last year in August Bogdanovski et al published Antibacterial activity of high-dose nitric oxide against pulmonary Mycobacterium abscessus disease. They describe a protocol of providing 30 minute doses of 160 ppm for 21 days in a 24 year old patient with cystic fibrosis who was infected with mycobacterium abscessus. While they were not able to eradicate the organism, they were able to demonstrate functional improvement in the patient. Also notable was the absence of adverse effects in terms of methemoglobin levels. Other prior research in-vitro has shown iNO at high levels to be truly bacteriocidal as per the review above.
In this paper they describe the use of iNO at 160 ppm in 5 spontaneously breathing patients with confirmed COVID19 infection. This was provided as a rescue therapy in the absence of any high quality therapies for this disease. The protocol was to give them the same dose of 160 ppm for 30 minutes at a time until resolution of their symptoms with those that received multiple treatments getting anywhere from 5-9 courses. In each case after each 30 minute period the treating physicians measured levels of methemoglobin and nitrogen dioxide and found in each patient acceptable levels after these brief exposures.
Results
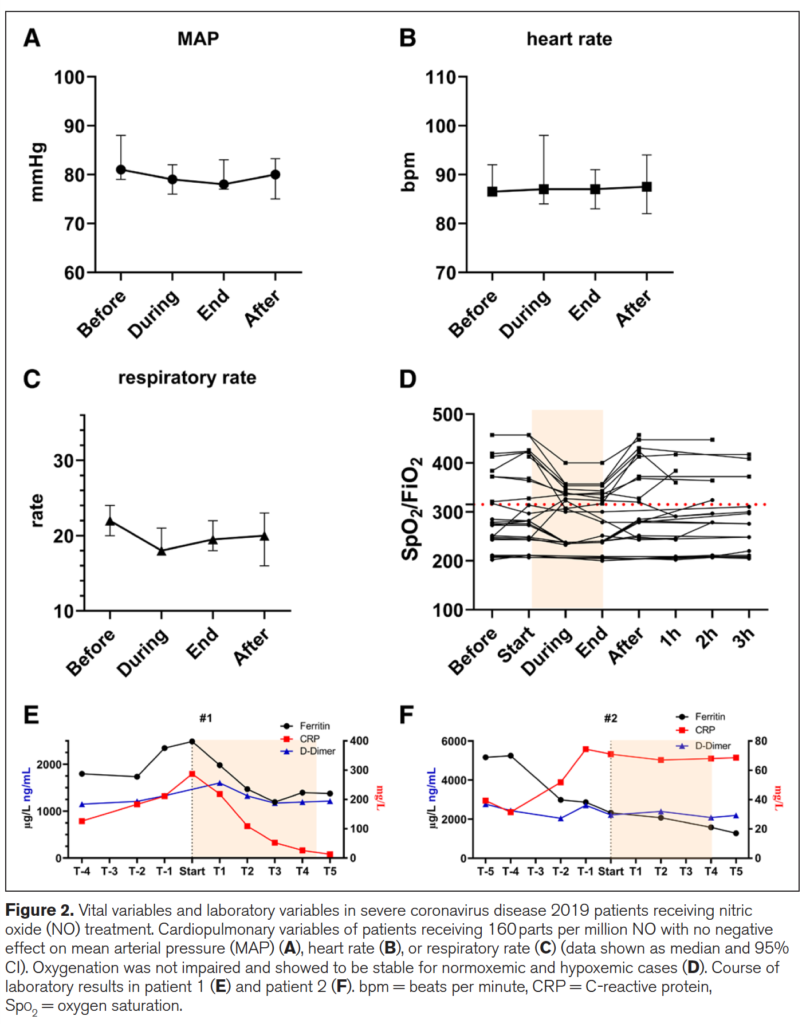
Of the 5 patients treated 2 died from COVID19 and three survived. The two patients who died interestingly were the ones who each only received one treatment each. The other three received 5, 8 and 9 treatments respectively. The authors recorded mean arterial pressure, heart rate, respiratory rate, SpO2/FiO2 and finally measurements of inflammatory markers in the two patients who died (E) and the 3 who survived in (F) in the figure below.
What is interesting from the figure above is the reduction in respiratory rate during treatment (certainly could be placebo from believing they will get better) but the oxygenation during the treatment improved as well. Could this be from a reduction in associated pulmonary hypertension? Certainly could be. Looking at the patients who died in (E) vs the ones in (F) who survived (patient 3 not shown) demonstrate that use of iNO stopped the rise in CRP and in the case of those who died reduced it significantly. There could be an argument made then that the changes in respiratory pattern observed during treatment are associated with a concomitant attenuation of inflammation. This treatment just might work but of course needs far more studies to be certain of that. On that note a review of iNO for this type of indication reveals there are currently 16 studies enrolling in this area of research so I imagine there will be more info to come with this story.
What about the neonate with pneumonia?
I sent this paper around to my colleagues and it generated some great discussion. I am no Ethicist but the question raised was could this be considered a “last ditch” treatment for the neonate succumbing to a pneumonia? I have no doubt if you are reading this that you will have seen in neonatal units around the world that there are infants who develop pneumonia unresponsive to traditional treatments such as iNO at regular doses, antibiotics, higher PEEP, surfactant etc. If we have this knowledge with respect to the potential use of iNO at high dose and a positive impact on pulmonary infective disease is this something that should be offered to parents?
We have no date to my knowledge in babies on the use of this type of dosing but it comes down to a question of what is the alternative? If a patient is dying on the ventilator are we at the point of knowledge here that it is worth offering the family this treatment? One could do so with full disclosure about the lack of neonatal data both for effectiveness and safety. Or do you fall on the side of it could be harmful and expedite death so should not be used. If you use it though and wait till the patient is in extremus on 100% oxygen might it be too late? Do parents have the right to know when they ask the question “is there anything else you can do?” For me I think the answer is that there should be a discussion with this evolving research out there. I am comfortable with it as long as the parents understand the potential for it to make things worse and shorten their time with their child. Alternatively if they choose not to that is their prerogative but should they have the choice when the competing outcome is death?
I can’t tell you whether you should or shouldn’t offer this in your institution but my suspicion is that you will be discussing this among colleagues before long. Who knows you might just one day say you saw it here first!
Thanks John M for the inspiration and keep sending those articles!
I had the pleasure of meeting the author of a paper I am about to comment on this week while at the 99 NICU conference in Stockholm. Dr. Ohlin from Orebro University in Sweden presented very interesting work on their unit’s “scrub the hub” campaign. As he pointed out, many places attempt to reduce coagulase negative staphylococcal infections by introducing central line bundles but seldom is there one thing that is changed in a bundle that allows for a before and after comparison like his team was able to do. I was so impressed by this work and at the same time concerned about another strategy to reduce infection that I felt compelled to make a comment here.
Scrub the hub!
Dr. Ohlin and the first author Dr. Bjorkman published Scrubbing the hub of intravenous catheters with an alcohol wipe for 15 sec reduced neonatal sepsis back in 2015. They compared a 16.5 month period in their unit when they rolled out a CLABI reduction bundle to a period of 8.5 months afterwards when they made one change. Nurses as is done in the units I work in were commonly scrubbing the hub before they injected the line with a medication but in the second epoch the standard changed to be a specified 15 second scrub instead of being left up to the individual nurse. With permission from Dr. Ohlin here is a picture of the hubs highlighting bacterial growth without scrubbing, then for a duration less than 15 seconds and then with 15 seconds.
In the first epoch they had 9 confirmed CLABSIs and 0 confirmed in the second after their intervention. The rate of CLABSI then in the first epoch was 1.5% vs 0% in the second group. As with any study looking at sepsis, definitions are important and while they didn’t do paired cultures to rule out contamination (one positive and one negative as is the definition in our hospitals) they did refer each patient to a senior Neonatologist to help determine whether each case should be considered a true positive or not. Given that they made no changes to practice or other definitions in diagnosing infections during that time perhaps the results were indeed real. Presumably if they had missed an infection and not treated it in the second epoch the patient would have declared themselves so I think it is reasonable to say that 8.5 months without a CLABSI after their intervention is a success. As Dr. Ohlin points out the scrub duration may also help due to the abrasion of the hub surface removing a bacterial film. Regardless of the reason, perhaps a 15 second scrub is a good idea for all?
The lazy person’s solution – the SwabCap
One way to get around human nature or people being distracted might be to cover each luer lock with a cap containing 70% isopropyl alcohol. In this way when you go to access the line there should be no bacteria or labour required to scrub anything since the entry of the line is bathed in alcohol already. This was the subject of a systematic review from the Netherlands entitled Antiseptic barrier cap effective in reducing central line-associated bloodstream infections: A systematic review and meta-analysis. The reviews ultimately examined 9 articles that met their inclusion criteria and found the following; use of the antiseptic barrier cap was effective in reducing CLABSIs (IRR = 0.59, 95% CI = 0.45–0.77, P < 0.001). Moreover, they concluded that this was an intervention worth adding to central-line maintenance bundles. Having said that, the studies were mostly adult and therefore the question of whether minute quantities of isopropyl alcohol might be injected with medications was not a concern when they made their conclusion.
What about using such caps in ELBW infants
Sauron et al in St. Justine Hospital in Montreal chose to look at these caps more carefully after they were implemented in their NICU. The reason for taking a look at them was due to several luer valves malfunctioning. The authors created an in-vitro model to answer this question by creating a closed system in which they could put a cap on the end of a line with a luer lock and then inject a flush, followed by a simulated medication (saline) and then a flush and collect the injected materials in a glass vial that was sealed to prevent evaporative loss of any isopropyl alcohol. They further estimated the safe amount of isopropyl alcohol from Pediatric studies would be 1% of the critical threshold of this alcohol and using a 500g infant’s volume of distribution came up with a threshold of 14 mmol/L. The study then compared using the SwabCap over two different valve leur lock systems they had in their units (SmartSite and CARESITE valves) vs. using the strategy of “scrub the hub”.
The results were quite concerning and are shown below.
Circuit Type
Temperature
Sample 1
Sample 2
Sample 3
Mean
SwabCap on Smart Site Valve
Room
49.5
58.4
46.8
51.6
Incubator 35 degrees
45.16
94.7
77.9
72.6
SwabCap on CARESITE valve
Room
14.1
5.7
5.2
8.34
Incubator 35 degrees
7.0
8.1
5.9
7.0
Isopropyl alcohol pad on CARESITE Valve
Room
0
0
0
0
Certainly, the Smart Site valve allowed considerable amounts of isopropyl alcohol to enter the line but the CARESITE while better still allowed entry compared to the control arm which allowed none. Beyond the introduction of the alcohol into the system in all cases considerable clouding of the valves occurred with repeated capping of the system with new caps as was done with each med injection since each was single use. In lines that were not accessed contact with the cap was left for 96 hours as per recommendations from the manufacturer and these changes occurred as well.
Conclusion
While a reduction in CLABSI is something we all need to strive to obtain, it is better to take the more difficult path and “scrub the hub” and by that for 15 seconds which incidentally is the same recommended duration for hand hygiene in both of our units. Perhaps in larger term infant’s seepage of isopropyl alcohol into the lines would not be as concerning as their larger volume of distribution would lead to lower levels but I would ask the question “should any isopropyl alcohol be injected into any baby?”. I think not and perhaps by reading this post you will ask the same thing if your unit is using these caps.
Thank you to Örebro University Hospital for their permission in using the photo for the post
I have been a huge advocate of RSV prophylaxis since my days as a Pediatric resident. When I started my residency we were not using Palivizumab (Synagis) and I recall admitting 10+ patients per day at times with bronchiolitis. With the use of passive immunization this rate dropped dramatically in Manitoba although rates in other areas of the country may have not seen such significant impacts. Manitoba may be somewhat different from many areas due to the communities in Nunavut being so impacted when RSV enters these areas and can infect many of the children due to crowded living conditions and inability to really isolate kids from one and other. The lack of benefit in other areas though, has no doubt led to controversy among practitioners who often wonder if giving 5 IM injections during the RSV season is indeed worth it. The real question has not necessarily been does it work but to whom should it be given so that you get the most benefit.
A Big Change in The Last Year
In 2015 the CPS published a revised statement entitled Preventing hospitalizations for respiratory syncytial virus infection. This statement has caused a great deal of controversy at least among those I have spoken with due to its significant departure from the previous recommendations. As per the statement:
In preterm infants without CLD born before 30 + 0 weeks’ GA who are <6 months of age at the start of RSV season, it is reasonable (but not essential) to offer palivizumab. Infants born after 30 + 0 weeks’ GA have RSV admission rates that are consistently ≤7% (Figure 3), yielding a minimum number needed to treat of 18 (90 doses of palivizumab to prevent one RSV admission) if one assumes 80% efficacy and five doses per infant. Therefore, palivizumab should not be prescribed for this group.
Gone are recommendations for treating those from 30 – 32 weeks and moreover 33- 35 weeks if meeting certain conditions. There is a provision for those in Northern communities to expand these criteria to 36 0/7 weeks if such infants would require medical transport to receive care for bronchiolitis. What is not really clear though is what is meant by Northern communities in terms of criteria to determine suitability exactly. Incidentally, the criteria are not so different than the AAP statement from August 2014.
Do We Need So Many Shots?
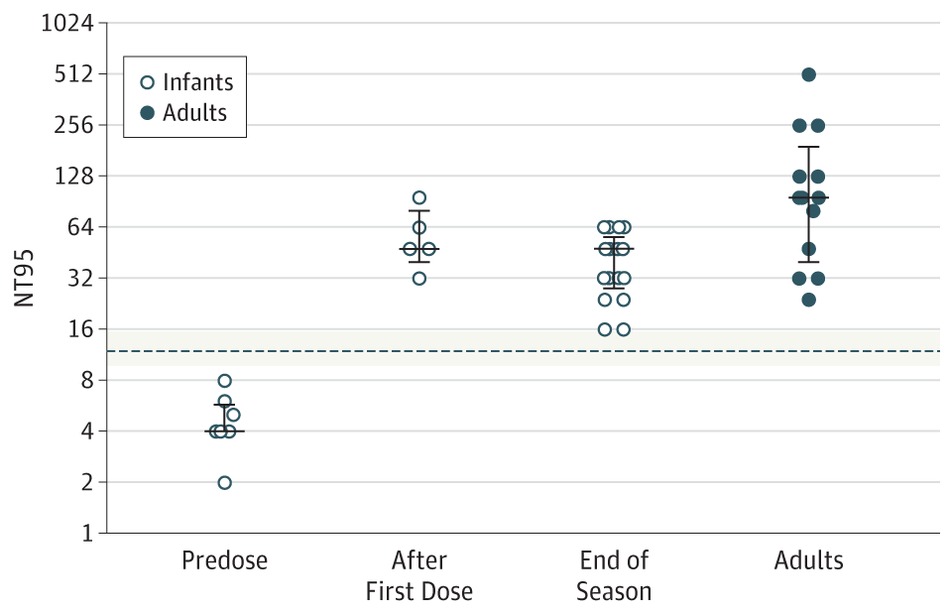
Just at the end of 2016 though Lavoie P et al in Vancouver, BC published a letter outlining their experience with a modified schedule of either 3 or 4 doses of palivizumab during the RSV season. Included in the letter are their criteria for determining the number of doses and importantly pharmacokinetic data demonstrating the effectiveness of such schedules in achieving protective titres. The 3 dose schedule was used for those infants born between 29 0/7 and 35 weeks gestational age who had a risk factor score of 42 or more. Interestingly at the end of the RSV season, depriving such infants of 1 or 2 doses did not appear to impair the ability of the infant to maintain protective levels.
From a clinical standpoint the outcome data during this period examining 514 (3 dose) and 666 (4 dose) patients similarly suggests that they were indeed protected from disease. In the 3 dose cohort only 1 patient was hospitalized with RSV during the dosing period and 1 infant afterwards. In the 4 dose group, 10 were hospitalized with RSV during the dosing schedule and a set of twins afterwards. Aside from these known RSV infections, an additional 7 and 18 patients were hospitalized with bronchiolitis without viral identification during the dosing schedule with no cases of bronchiolitis afterwards. Taken altogether and assuming that all cases were indeed RSV bronchiolitis the authors conclude that the overall rates are no different than those seen with a 5 dose schedule.
Is Something Rotten In The State of Denmark?
There is something peculiar here though. There is no doubt that palivizumab must have gone through rigorous pharmacokinetic testing in order to determine the correct number of doses needed. For a 3-4 dose regimen to provide the same coverage in terms of antibody titres seems strange to me. I would love to believe the data but there is a skeptic in me. Secondly with respect to counting hospital admissions is this exhaustive in terms of including all hospitalization a in BC or at only some sites? Clarity is needed before considering such changes to practice. Strangely it has been several months since this experience was published and there has been no discussion of it at least locally.* Something as dramatic as this should have sparked some discussion and the absence of such leaves me questioning what am I missing?
From the standpoint of reducing interventions and pain in the neonate I am intrigued by these findings. Parents as well would no doubt be happier with 3-4 IM injections over 5. The additional benefit is no doubt financial as this product while effective does carry a significant cost per dose. As you can see I have my doubts about the reproducibility of the results but it does at least offer some centres that have not been as enthusiastic about palivizumab something to consider. For some, the BC approach just might be the right thing.
I indicate that there has been little discussion locally of the article discussed. There has indeed been discussion both here and in other Canadian provinces. What I meant by that comment is that among my colleagues in Neonatology and Infectious Diseases and housestaff I have had only one discussion.
It is one of the first things that a medical student pledges to do; that is to do no harm. We are a fearful lot, wanting to do what is best for our patients while minimizing any pain and suffering along the way. This is an admirable goal and one which I would hope all practitioners would strive to excel at. There are times however when we can inadvertently cause more harm than good when we try to avoid what we perceive is the greater harm.
This is the case when it comes to collecting a sample of urine for culture as part of a full septic workup. If you ask most healthcare providers they will freely acknowledge that the gold standard for determining whether an infant has a UTI is a supra pubic aspirate (SPA). We so rarely do them these days however due to a whole host of reasons. Problems with collection include the timing and accuracy of needle placement both of which may often lead to an empty tap. Secondly after a number of missed attempts and a crying infant who appears to be in pain it is understandable why bedside nurses may become frustrated with the entire experience and urge the person performing such procedures to settle on a bladder catheterization (BC) to obtain the specimen.
All in all the BC performed quite poorly when compared to the gold standard. The false positive rate compared to SPA was 71.1%! That is to say that only 28.9% of SPA samples were positive compared to BC. Similarly urinalysis sensitivity and specificity from BC were 66.7% (95% CI, 44.68% to 84.33%) and 93.22% (95% CI, 83.53% to 98.08%), respectively. This means that only 2/3 of the time was the urinalysis abnormal on a BC in the presence of a true UTI. Somewhat reassuring is that when there really was no UTI the urinalysis was mostly negative but in almost 1/10 patients it would not by itself rule out a UTI.
What Is The Harm in Continuing BC Instead of SPA?
When we try to avoid the perceived painful experience of a SPA we are going to wind up treating a large number of patients for a presumed UTI who don’t have one. The harm in this is the exposure of such infants to prolonged courses of antibiotics which has been a subject discussed many times over on this site. We put our patients at risk of antibiotic resistance and shifts in the gut microbiome which in the case of the preterm infant puts them at risk of necrotizing enterocolitis. There are many other concerns with prolonging antibiotics but these few should be reason enough to strive for accuracy in obtaining the right specimen in the right way. Putting it in a slightly different perspective, would you settle for an alternative test to a lumbar puncture which claimed to miss 1 in 10 cases and also found meningitis where there was none 71.1% of the time?!
A Way Forward – A Recipe For Success
As the saying goes, measure twice and cut once. With the use of bedside ultrasound there should be no need to guess as to whether the bladder is full or not. Secondly the placement of the needle should no longer need to rely on landmarking but actually seeing where the best place for needle placement is. Assessing the bladder by ultrasound is easy and is already employed at the bedside by nurses in many areas of the hospital. There should no longer be a reason for the empty tap as the practitioner can be called when the baby is ready as evidenced by a good amount of urine in the bladder.
Given that we have some time to do the blood culture and LP, while we wait for the SPA to be done either sucrose in the premature infant or IV analgesic may be given for the SPA while in the term or older infant there is an opportunity to put a topical analgesic cream over the site. There really is little need for pain to factor into this any longer.
Ask any health care provider and they will tell you they want to do the best they can for their patient. This study shows us that performing a BC is failing to meet that goal. We need to change our ways and return to the practice of the SPA but this time we have to get it right.




 The 3 dose schedule was used for those infants born between 29 0/7 and 35 weeks gestational age who had a risk factor score of 42 or more. Interestingly at the end of the RSV season, depriving such infants of 1 or 2 doses did not appear to impair the ability of the infant to maintain protective levels.
The 3 dose schedule was used for those infants born between 29 0/7 and 35 weeks gestational age who had a risk factor score of 42 or more. Interestingly at the end of the RSV season, depriving such infants of 1 or 2 doses did not appear to impair the ability of the infant to maintain protective levels.