Throughout my career one thing has been consistently true. That is that wherever I was working and regardless of the role I have been an educator. I imagine the blog to a great extent is related to my interest in this aspect of my work. In the last few years much has been said about care by parents whether it be a general approach for family centred care or in formalized approaches such as FiCare which has also been formally studied in the research setting. When we speak of family centred care, one thing that I am constantly reminded of is that the focus of all of our efforts must be on the family and the patient. As I said recently to a colleague when discussing what was presented as a difficult discussion with another colleague due to a disagreement about the direction of management, when you put the patient first the discussion really isn’t difficult at all. It’s not about you or a colleagues ego but about the patient and if the management is not up to par then change direction and worry about managing egos later.
What We Know And What They Know
Another aspect that needs to be addressed is the difference in power that we have through knowledge. I am not talking about us exerting authority over families but from the perspective of us having the knowledge from years of experience in the field as to what is significant and what is not in terms of events in the NICU. The evidence for example with respect to neurodevelopmental outcome from apnea and bradycardia should give us reason to be optimistic the majority of the time. While in Edmonton I learned a great deal from one of my colleagues who was the lead author in a paper entitled Early childhood neurodevelopment in very low birth weight infants with predischarge apnea. While frequent apnea may be associated with mild motor impairments in their paper, the predictive value of these predischarge recordings is very limited when you take away those kids without severe IVH. I think about all of the parents we see who have their eyes glued to the monitors while they attend at the bedside and what they must be thinking. To us it is just a matter of time but I wonder for them how agonizing a time it really is! It isn’t just those infants who are nearing discharge and having apnea either as the CAP study at 5 years of age showed no difference in survival without disability in those infants who received caffeine vs those who did not. More frequent events may not be that detrimental after all. I am not suggesting we not treat patients as one never knows where the threshold lies to cause injury but these preemies are certainly made of some tough stuff.
Identifying Stress and Preparing Parents For it
The first step in dealing with this issue is to know it is there. Recognizing this, Melnyk and others performed an educational intervention targeting behaviour of families in their study Reducing premature infants’ length of stay and improving parents’ mental health outcomes with the Creating Opportunities for Parent Empowerment (COPE) neonatal intensive care unit program: a randomized, controlled trial. The group of parents who went through the program had better mental health outcomes compared to the control groups. The issue here and really is at the crux of the goal in writing all of this is that the stress that parents feel may not be overtly present. The squeaky wheel as the saying goes gets the grease and the parents that are demonstrating signs of poor coping are the first to draw the referrals to social work or engage in a deeper conversation with nursing at the bedside. All parents experience stress at least to a certain degree and it is all of our jobs to tease it out. On the other hand employing standardized approaches such as the COPE program for all parents might be another way of helping those who are in need but not clearly wearing a sign on their foreheads that say “help me”.
Don’t Underestimate the Power of Reassurance
So we know that much of what we see on the monitors will not lead to long term harm, transient central cyanosis during feeds will not damage the brain and apnea of prematurity is a distinct entity from SIDS. The parents on the other hand commonly make these links and additionally in case no one has mentioned it to you, those babies with TTN may one day develop asthma and those with hypoglycemia may have diabetes (we know both not to be true but I have been asked about this many times). This is why I believe it is our duty to explain why we are not worried about things that come up in the unit. Saying “don’t worry” or “that is normal preterm behaviour” may not be enough. Ask a parent what it is they are worried about and you may be surprised to find out the links that they have made in their heads, some of which may be valid but some completely false. I am not meaning to trivialize their concerns but rather validate them as real worries. If we have the knowledge and it is power as I said before then shouldn’t we use that power to help reduce their stress?
Engaging Families Can Reap Huge Dividends
The movement towards family centred care and more specifically care by parent will have a dramatic impact on this issue. As more and more centres move to engaging families to be part of rounds and not just listen and then ask questions but to take some degree of control and provide some of the reporting stress will be reduced. It is only logical. The more a family comes to understand what is significant and what is not in terms of reporting concerns the more confident they will be. Moreover, spending more time at the bedside leads to more skin to skin care and with that shorter hospital stays due to better cardiorespiratory stability. We aren’t there yet but we are headed in the right direction. In the meantime, take the time to ask a simple question “what are you worried about” to parents no matter how confident and strong they appear and you may find yourself with an opportunity to harness the power of education you have a make a real difference to a family in need.
I have probably received more requests for our glucose gel protocol than any other question since I started writing on this blog. Dextrose gel has been used more and more often for treatment of hypoglycemia such that it is now a key strategy in the management of low blood sugar in ours and many other institutions. If you are interested in the past analyses of the supporting trials they can be found in these posts; Glucose gel For Managing Hypoglycemia. Can We Afford Not To Use It? and Dextrose gel for hypoglycemia: Safe in the long run? As you can tell from these posts I am a fan of dextrose gel and eagerly await our own analysis of the impact of using gel on NICU admission rates for one!
But What If You Could Prevent Hypoglycemia Rather Than Treating It?
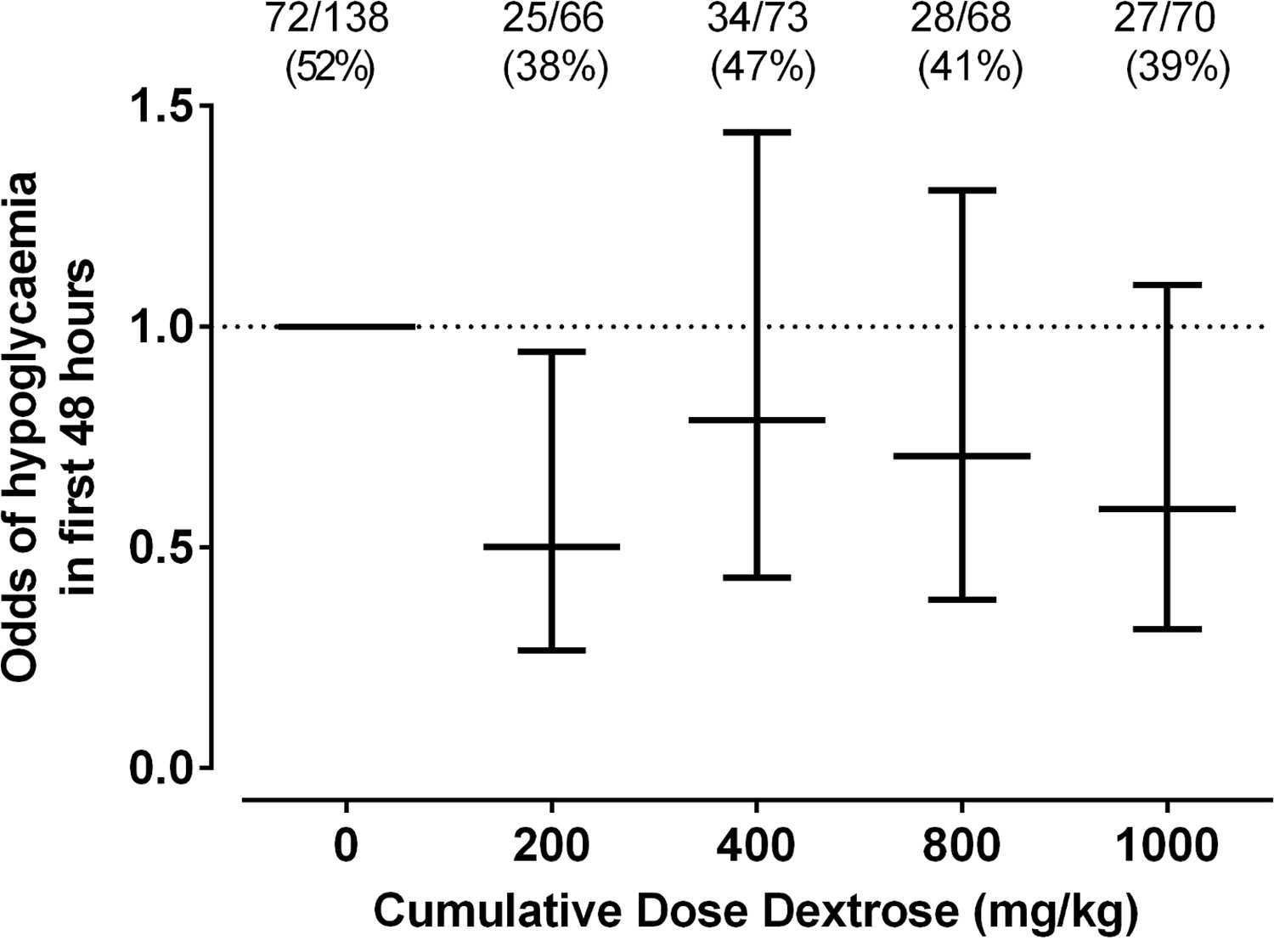
This is the question that the same group who has conducted the other trials sought to answer in their dose finding study entitled Prophylactic Oral Dextrose Gel for Newborn Babies at Risk of Neonatal Hypoglycaemia: A Randomised Controlled Dose-Finding Trial (the Pre-hPOD Study). I suppose it was only a matter of time that someone asked the question; “What if we prophylactically gave at risk babies dextrose gel? Could we prevent them from becoming hypoglycemic and reduce admissions and improve breastfeeding rates as has been seen with treatment of established hypoglycemia?” That is what they went out and did. The group selected at risk patients such as those born to mothers with any type of diabetes, late preterm infants, SGA and others typically classified as being at risk but who did not require NICU admission at 1 hour of age when treatment was provided. The primary outcome was hypoglcyemia (<2.6 mmol/L) in the first 48 hours. Secondary outcomes included NICU admissions, breastfeeding rates in hospital and after discharge as well as formula intake at various time points.
The study sought really to serve as a pilot whose goal was to determine when compared to placebo whether several different regimens could prevent development of hypoglycemia. The groups were (with the first dose in each case given at 1 hour of age):
Single dose of 40% dextrose gel – 0.5 mL/kg
Single dose of 40% dextrose gel – 1 ml/kg
Four doses of 0.5 mL/kg given every three hours with breastfeeding
A single dose of 1 mL/kg then 3 X 0.5 mL/kg given q3h before each breastfeed.
In total 412 patients were randomized into 8 different groups (4 treatment and 4 placebo).
As The Saying Goes, Less Is More
The only dose of dextrose that reduced the risk of hypoglycemia in the first 48 hours was 0.5 mL/kg which provides 200 mg/kg of dextrose which is the same as a bolus of IV dextrose when giving 2 mL/kg of D10W. Curiously using a higher dose or using multiple doses had no effect on reducing the risk. Based on a difference of 14% between placebo and this group you would need to treat roughly 7 patients with dextrose gel once to prevent one episode of hypoglycemia. Also worth noting is that admission to NICU was no different but if one restricted the reason for admission to hypoglycemia the difference was significant (13% vs 2% risk; p = 0.04). What was not seen here was a difference in rates of breastfeeding and much effect on use of formula.
Why Might These Results Have Occurred?
Insulin levels were not measured in this study but I truly wonder if the reason for hypoglycemia in the other groups may have been transient hyperinsulinemia from essentially receiving either a very large load of glucose (1 mL/kg groups) or effectively 4 boluses of glucose in the first 12 hours of feeding. Rebound hypoglycemia from IV boluses is a known phenomenon as insulin levels surge to deal with the large dextrose load and I can’t help but wonder if that is the reason that all but the single dose regimen had an effect. It is also worth commenting that with so many secondary outcomes in this study the p values needed to reach significance are likely much smaller than 0.05 so I would take the reduction in NICU admissions for hypoglycemia with a grain of salt although at least the trend is encouraging.
I wouldn’t change my practice yet and the authors do acknowledge in the article that a much larger study is now being done using the single dose of 0.5 mL/kg to look at outcomes and until that is published I don’t think a practice change is in order. What this study does reinforce though is that providing multiple doses of dextrose gel may yield diminishing returns. While the goal here was prophylaxis, I can’t help but think about the patients who are symptomatic and receive two or three gels and still wind up with an IV. Could it be the same rebound hypoglycemia at play?
We also have to acknowledge that even if this is an effective preventative strategy, is it in the best interests of the babies to all receive such treatment when at least in 6 babies they wouldn’t have needed any? Could such treatment simply be reserved as has been done for those who develop hypoglycemia? Those who question the safety of the ingredients such as dyes that are found in the product may want some long term safety data before this becomes routine in at risk babies but it won’t surprise me if such strategies become commonplace pending the results of the larger trial on the way.
The other day I met with some colleagues from Obstetrics and other members from Neonatology to look at a new way of configuring our delivery suites. The question on the table was which deliveries which were always the domain of the high risk labour floor could be safely done in a lower acuity area. From a delivery standpoint they would have all the tools they need but issues might arise from a resuscitation point of view if more advanced resuscitation was needed. Would you have enough space for a full team, would all the equipment you need be available and overall what is in the best interests of the baby and family?
We looked at a longstanding list of conditions both antenatal and intrapartum and one by one tried to decide whether all of these were high risk or if some were more moderate. Could one predict based on a condition how much resuscitation they might need? As we worked our way through the list there was much discussion but in the end we were left with expert opinion as there was really no data to go by. For example, when the topic of IUGR infants came up we pooled our collective experience and all agreed that most of the time these babies seem to go quite well. After a few shoulder shrugs we were left feeling good about our decision to allow them to deliver in the new area. Now several days later I have some concern that our thinking was a little too simple. You see, conditions such as IUGR may present as the only risk factor for an adverse outcome but what if they also present with meconium or the need for a instrument assisted delivery. We would presume the risk for advanced resuscitation (meaning intubation or chest compressions and/or medication need) would be increased but is there a better way of predicting the extent of this risk?
Indeed there might just be
An interesting approach to answer this question has been taken by an Argentinian group in their paper Risk factors for advanced resuscitation in term and near-term infants: a case–control study. They chose to use a prospective case control study matching one case to 4 control infants who did not require resuscitation. The inclusion criteria were fairly straightforward. All babies had to be 34 weeks gestational age or greater and free of congenital malformations. By performing the study in 16 centres they were able to amass 61953 deliveries and for each case they found (N=196) they found 784 deliveries that were matched by day of birth. The idea here was that by matching consecutive patients who did not require resuscitation you were standardizing the teams that were present at delivery.
The antepartum and intrapartum risk factors that were then examined to determine strengths of association with need for resuscitation were obtained from the list of risks as per the NRP recommendations.
A Tool For All of Us?
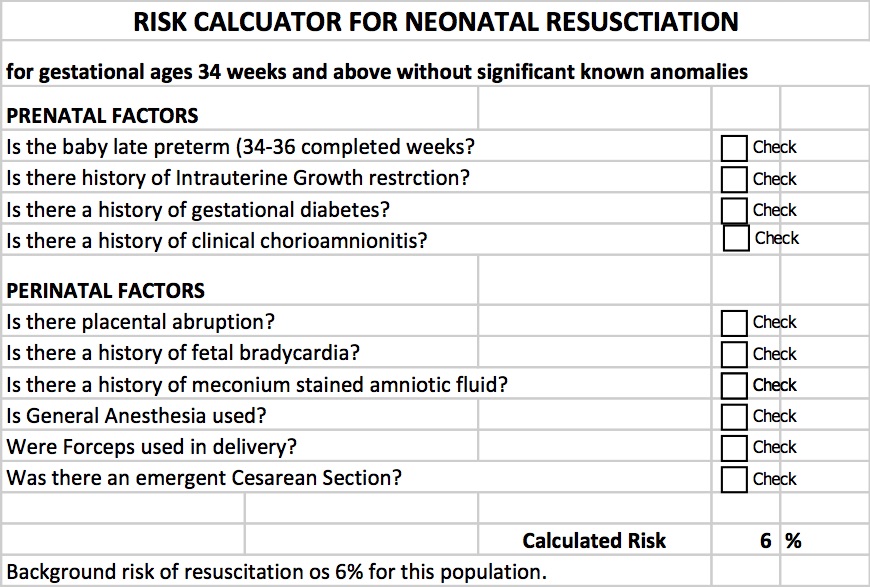
What came out of their study was a simple yet effective tool that can help to predict the likelihood of a baby needing resuscitation when all factors are taken into account. By resuscitation the authors defined this as intubation, chest compressions or medications. This is pretty advanced resuscitation! In essence this is a tool that could help us answer the questions above with far better estimation than a shoulder shrug and an “I think so” response. The table can be found by clicking on this link to download but the table looks like this.
By inserting checks into the applicable boxes you get a calculated expected need for resuscitation. Let’s look at the example that I outlined at the start of the discussion which was an IUGR infant. It turns out that IUGR itself increases the background risk for infants 34 weeks and above from 6% to 55% with that one factor alone. Add in the presence of fetal bradycardia that is so often seen with each contraction in these babies and the risk increases to 97%! Based on these numbers I would be hesitant to say that most of these kids should do well. The majority in fact would seem to need some help to transition into this world.
Some words of caution
The definition here of resuscitation was intubation, chest compressions or medications. I would like to presume that the practioners in these centres were using NRP so with respect to chest compressions and medication use I would think this should be comparable to a centre such as ours. What I don’t know for sure is how quickly these centres move to intubate. NRP has always been fairly clear that infants may be intubated at several time points during a resuscitation although recent changes to NRP have put more emphasis on the use of CPAP to establish FRC and avoid intubation. Having said that this study took place from 2011 – 2013 so earlier than the push for CPAP began. I have to wonder what the effect of having an earlier approach to intubating might have had on these results. I can only speculate but perhaps it is irrelevant to some degree as even if in many cases these babies did not need intubation now they still would have likely needed CPAP. The need for any respiratory support adds a respiratory therapist into the mix which in a crowded space with the additional equipment needed makes a small room even smaller. Therefore while I may question the threshold to intubate I suspect these results are fairly applicable in at least picking out the likelihood of needing a Neonatal team in attendance.
Moreover I think we might have a quick tool on our hands for our Obstetrical colleagues to triage which deliveries they should really have us at. A tool that estimates the risk may be better than a shoulder shrug even if it overestimates when the goal is to ensure safety.
This is a posting of an article in Pediatrics. Always wondered whether this little venture of mine would be studied. Not this blog in particular but the whole concept in general! The credit of course for this post is not mine but Dr. Moreno who wrote the piece but as the link wouldn’t work well on the Facebook page independently here you go.
Mastering the Media: Physician bloggers identify benefits, barriers to using social media
Megan A.Moreno, M.D., M.S.Ed., M.P.H., FAAP
Dr. Moreno
A growing number of physicians use social media as a professional platform for health communication. This trend is not lost on medical students and residents, who are among the demographic described as “most connected” via social media.In 2014, a medical student asked me to serve as her mentor for a public health research project. The student, Lauren Campbell, was interested in studying how physician bloggers see themselves and their role as bloggers, as well as the benefits and risks of blogging as a doctor. Given the newness of physician blogging, the purpose of the study was to understand the perspectives and experiences of physicians who could be considered early adopters of using social media to distribute health information.
We recruited physicians to take part in the study through website searches for physician bloggers, and in-depth telephone interviews were conducted with those who agreed to participate. At the end of the interview, participants were asked if they could recommend other physician bloggers, a technique known as “snowball sampling.”
Seventeen physicians participated in the study, which recently was published in BMC Medical Informatics and Decision Making (http://bit.ly/2bFtno9). About one-third were female and 76% were pediatricians.
Transcripts were analyzed for common themes mentioned across interviews.
Participants identified multiple perceived benefits and barriers to social media use by physicians. Benefits included forwarding career endeavors, keeping up with medical literature and increasing public exposure for their practice. Barriers included time, administrative hurdles to get permission from their institution to blog and fear of saying the wrong thing.
In addition, four major themes were commonly discussed across interviews. First, participants often saw themselves as “rugged individualists” who set their own rules for social media health communications, like cowboys taming the Wild West.
Second, participants expressed uncertainty about boundaries and strategies for social media use. They identified many gray areas such as what to post, how to post and how to set boundaries.
Third, an interesting and unexpected finding was that most of the physician bloggers described using social media much like traditional media, as a one-way communication platform or “soapbox” rather than as an interactive forum.
Finally, participants had disparate views regarding the time involved in social media use; some felt they could fit blogging into their day, while others saw it as an impediment to patient care.
From this study, we concluded that much uncertainty remains regarding roles and responsibilities of physicians providing medical content within social media, and opportunities exist for providers to use social media platforms interactively and to their full potential.
It’s worth considering how the AAP Council on Communications and Media or the Academy could develop best practices to address some of this uncertainty and provide physicians with training or tools to use social media for its true interactive purpose. The hope is that future studies will investigate these key topics so the “Wild West” of physician blogging will become an integrated metropolis.
Dr. Moreno is a member of the AAP Council on Communications and Media Executive Committee.
Campaign Closed October 13,2016! Thank you everyone for the $9359.00 raised!
Each day the number of people following these sites grows and at the time of this post, the largest following on Facebook has over 8200 people who receive the feed on a daily basis. That is nothing short of remarkable and I hope that each of you gets something out of my writings and postings. I recognise that each post may not “light it up” in your mind but if you get at least a few “a ha” moments along the way then I am very happy that you have found these sites!
What This Is Not!
As I begin hinting at money, many of you may be thinking “here we go”, he is finally asking for some payment for this site! To be clear I have no interest in personal financial gain from this hobby I have developed, but rather find my joy in sharing ideas, getting your feedback and helping to generate interest overall in topics pertaining to Neonatology. I have no intention of ever asking for such payment but that doesn’t mean that I might not want to help someone else. For those of you who make philanthropy a part of your lives you will know the joy that comes from helping others. Being able to help others need not take tremendous dollars per donor when you have many people banding together to help a cause. This is the power that I am hoping to harness through this initiative and make a difference in care to our babies in hospital.
For the past year and a half, I have put my fingers to the keyboard to hopefully share my knowledge and expertise with you about an industry I am so passionate about.
My Philanthropic Side
When I am not busy finding content for the sites or being a Neonatologist, I am quite dedicated to philanthropy. One thing people may not realise about our province/country is that the government helps out the best they can financially but with the heavy demands of our province, they can’t meet all the needs. That’s why I’m proud of my partnership with the Children’s Hospital Foundation of Manitoba. The Foundation’s donors have helped bridge the gap so our hospital doesn’t go without the specialised items they need. From ultrasounds, starting a breast milk depot, specialised pediatric equipment and funding a position to support Quality Improvement in our unit to a soon to be announced Family Support coordinator position and so much more. But now, I turn to you to help us make the next difference in our unit.
The other day as the Facebook page hit 8,000 followers a thought struck me. What if I asked everyone on the page to just give $1 towards the purchase of a piece of equipment for babies in our units?
Hold Their Hand
In the Neonatal Intensive Care Unit (NICU), they are watched closely to make sure they are getting the right balance of fluids and nutrition. Incubators or special warmers help babies maintain their body temperature. This reduces the energy the babies have to use to stay warm and allow them to use that energy elsewhere.
Premature babies need to receive good nutrition so they grow at a rate close to that of babies still inside the womb. Babies born under 38 weeks have different nutritional needs than babies born at full term (after 38 weeks). They often have problems feeding from a bottle or a breast. This is because they are not yet mature enough to coordinate sucking, breathing, and swallowing.
Many NICUs will give donor milk from a milk bank to high-risk babies who cannot get enough milk from their own mother. But because the baby must be kept at a certain temperature to stay warm, so does their milk.
Thanks to the generous support of donors to the Children’s Hospital Foundation of Manitoba, 12 milk warmers have been purchased. However, we need 24 more warmers to keep up with demand. Each one costs $2,000 and will make a huge impact. An impact to help our babies get the nutrition they need at the temperature they require to survive and thrive.
So let’s hold their hand and let’s do it together! Has this journey of learning been worth at least $1 to you? If it has, then please help make a difference by giving at least $1. Giving more will only increase the power of this campaign! If you aren’t able to donate $1 or more, I ask that you share this post and challenge your friends to help make a difference to the over 1,000 patients we see a year. Click the link below to donate and make your difference today.
I have been a huge advocate of RSV prophylaxis since my days as a Pediatric resident. When I started my residency we were not using Palivizumab (Synagis) and I recall admitting 10+ patients per day at times with bronchiolitis. With the use of passive immunization this rate dropped dramatically in Manitoba although rates in other areas of the country may have not seen such significant impacts. Manitoba may be somewhat different from many areas due to the communities in Nunavut being so impacted when RSV enters these areas and can infect many of the children due to crowded living conditions and inability to really isolate kids from one and other. The lack of benefit in other areas though, has no doubt led to controversy among practitioners who often wonder if giving 5 IM injections during the RSV season is indeed worth it. The real question has not necessarily been does it work but to whom should it be given so that you get the most benefit.
A Big Change in The Last Year
In 2015 the CPS published a revised statement entitled Preventing hospitalizations for respiratory syncytial virus infection. This statement has caused a great deal of controversy at least among those I have spoken with due to its significant departure from the previous recommendations. As per the statement:
In preterm infants without CLD born before 30 + 0 weeks’ GA who are <6 months of age at the start of RSV season, it is reasonable (but not essential) to offer palivizumab. Infants born after 30 + 0 weeks’ GA have RSV admission rates that are consistently ≤7% (Figure 3), yielding a minimum number needed to treat of 18 (90 doses of palivizumab to prevent one RSV admission) if one assumes 80% efficacy and five doses per infant. Therefore, palivizumab should not be prescribed for this group.
Gone are recommendations for treating those from 30 – 32 weeks and moreover 33- 35 weeks if meeting certain conditions. There is a provision for those in Northern communities to expand these criteria to 36 0/7 weeks if such infants would require medical transport to receive care for bronchiolitis. What is not really clear though is what is meant by Northern communities in terms of criteria to determine suitability exactly. Incidentally, the criteria are not so different than the AAP statement from August 2014.
Do We Need So Many Shots?
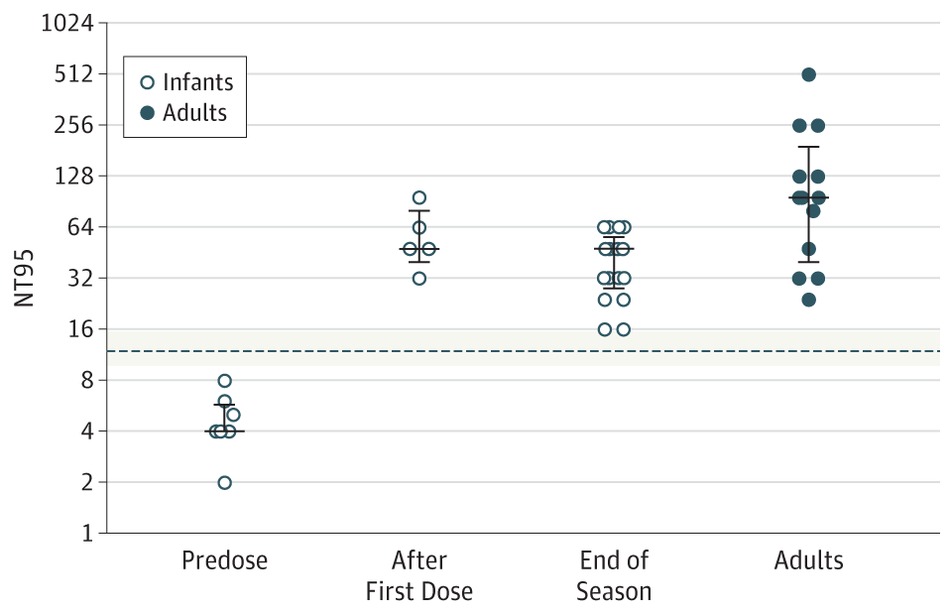
Just at the end of 2016 though Lavoie P et al in Vancouver, BC published a letter outlining their experience with a modified schedule of either 3 or 4 doses of palivizumab during the RSV season. Included in the letter are their criteria for determining the number of doses and importantly pharmacokinetic data demonstrating the effectiveness of such schedules in achieving protective titres. The 3 dose schedule was used for those infants born between 29 0/7 and 35 weeks gestational age who had a risk factor score of 42 or more. Interestingly at the end of the RSV season, depriving such infants of 1 or 2 doses did not appear to impair the ability of the infant to maintain protective levels.
From a clinical standpoint the outcome data during this period examining 514 (3 dose) and 666 (4 dose) patients similarly suggests that they were indeed protected from disease. In the 3 dose cohort only 1 patient was hospitalized with RSV during the dosing period and 1 infant afterwards. In the 4 dose group, 10 were hospitalized with RSV during the dosing schedule and a set of twins afterwards. Aside from these known RSV infections, an additional 7 and 18 patients were hospitalized with bronchiolitis without viral identification during the dosing schedule with no cases of bronchiolitis afterwards. Taken altogether and assuming that all cases were indeed RSV bronchiolitis the authors conclude that the overall rates are no different than those seen with a 5 dose schedule.
Is Something Rotten In The State of Denmark?
There is something peculiar here though. There is no doubt that palivizumab must have gone through rigorous pharmacokinetic testing in order to determine the correct number of doses needed. For a 3-4 dose regimen to provide the same coverage in terms of antibody titres seems strange to me. I would love to believe the data but there is a skeptic in me. Secondly with respect to counting hospital admissions is this exhaustive in terms of including all hospitalization a in BC or at only some sites? Clarity is needed before considering such changes to practice. Strangely it has been several months since this experience was published and there has been no discussion of it at least locally.* Something as dramatic as this should have sparked some discussion and the absence of such leaves me questioning what am I missing?
From the standpoint of reducing interventions and pain in the neonate I am intrigued by these findings. Parents as well would no doubt be happier with 3-4 IM injections over 5. The additional benefit is no doubt financial as this product while effective does carry a significant cost per dose. As you can see I have my doubts about the reproducibility of the results but it does at least offer some centres that have not been as enthusiastic about palivizumab something to consider. For some, the BC approach just might be the right thing.
I indicate that there has been little discussion locally of the article discussed. There has indeed been discussion both here and in other Canadian provinces. What I meant by that comment is that among my colleagues in Neonatology and Infectious Diseases and housestaff I have had only one discussion.


 So we know that much of what we see on the monitors will not lead to long term harm, transient central cyanosis during feeds will not damage the brain and apnea of prematurity is a distinct entity from SIDS. The parents on the other hand commonly make these links and additionally in case no one has mentioned it to you, those babies with TTN may one day develop asthma and those with hypoglycemia may have diabetes (we know both not to be true but I have been asked about this many times). This is why I believe it is our duty to explain why we are not worried about things that come up in the unit. Saying “don’t worry” or “that is normal preterm behaviour” may not be enough. Ask a parent what it is they are worried about and you may be surprised to find out the links that they have made in their heads, some of which may be valid but some completely false. I am not meaning to trivialize their concerns but rather validate them as real worries. If we have the knowledge and it is power as I said before then shouldn’t we use that power to help reduce their stress?
So we know that much of what we see on the monitors will not lead to long term harm, transient central cyanosis during feeds will not damage the brain and apnea of prematurity is a distinct entity from SIDS. The parents on the other hand commonly make these links and additionally in case no one has mentioned it to you, those babies with TTN may one day develop asthma and those with hypoglycemia may have diabetes (we know both not to be true but I have been asked about this many times). This is why I believe it is our duty to explain why we are not worried about things that come up in the unit. Saying “don’t worry” or “that is normal preterm behaviour” may not be enough. Ask a parent what it is they are worried about and you may be surprised to find out the links that they have made in their heads, some of which may be valid but some completely false. I am not meaning to trivialize their concerns but rather validate them as real worries. If we have the knowledge and it is power as I said before then shouldn’t we use that power to help reduce their stress?






 The 3 dose schedule was used for those infants born between 29 0/7 and 35 weeks gestational age who had a risk factor score of 42 or more. Interestingly at the end of the RSV season, depriving such infants of 1 or 2 doses did not appear to impair the ability of the infant to maintain protective levels.
The 3 dose schedule was used for those infants born between 29 0/7 and 35 weeks gestational age who had a risk factor score of 42 or more. Interestingly at the end of the RSV season, depriving such infants of 1 or 2 doses did not appear to impair the ability of the infant to maintain protective levels.