It seems like a sensational title I know but it may not be as far fetched as you may think. The pendulum certainly has swung from the days of liberal post natal dexamethasone use in the 1990s to the near banishment of them from the clinical armamentarium after Keith Barrington published an article entitled The adverse neuro-developmental effects of postnatal steroids in the preterm infant: a systematic review of RCTs in BMC Pediatrics in 2011. This article heralded in the steroid free epoch of the first decade of the new millennium, as anyone caring for preterm infants became fearful of causing lifelong harm from steroid exposure. Like any scare though, with time fear subsides and people begin asking questions such as; was it the type of steroid, the dose, the duration or the type of patient that put the child at risk of adverse development? Moreover, when death from respiratory failure is the competing outcome it became difficult to look a parent in the eye when their child was dying and say “no there is nothing more we can do” when steroids were still out there.
Over the last decade or so, these questions in part have been studied in at least two important ways. The first was to ask whether we use a lower dose of dexamethasone for a shorter period to improve pulmonary outcomes without adverse neurodevelopment? The target population here were babies on their way to developing chronic lung disease as they were ventilated at a week of age. The main study to answer this question was the DART study. This study used a very low total dose of 8.9 mg/kg of dexamethasone given over ten days. While the study was stopped due to poor recruitment (it was surely difficult to recruit after the 2001 moratorium on steroids) they did show a benefit towards early extubation. This was followed up at 2 years with no difference in neurodevelopmental outcomes. Having said that the study was underpowered to detect any difference so while reassuring it did not prove lack of harm. Given the lack of evidence showing absolute safety practitioners have continued to use post natal steroids judiciously.
The second strategy was to determine whether one could take a prophylactic approach by providing hydrocortisone to preterm infants starting within the first 24 hours to prevent the development of CLD. The best study to examine this was by Kristi Watterberg in 2004 Prophylaxis of early adrenal insufficiency to prevent bronchopulmonary dysplasia: a multicenter trial. Strangely enough the same issue of early stoppage affected this study as an increased rate of spontaneous gastrointestinal perforation was noted leading to early closure. The most likely explanation is thought to be the combination of hydrocortisone and indomethacin prophylaxis which some centres were using at the same time. An interesting finding though was that in a subgroup analysis, infants with chorioamnionitis who received hydrocortisone had less incidence of chronic lung disease. (more on this later) Although this of course is subject to the possible bias of digging too deep with secondary analyses there is biologic plausibility here as hydrocortisone could indeed reduce the inflammatory cascade that would no doubt be present with such infants exposed to chorioamnionitis in utero.
Has the answer finally come?
The DART study at 360 patients was the largest study to date to look at prophylaxis as a strategy. That is until this past week. The results of the PREMILOC study have been published which is the long awaited trial examining a total dose of 8.5 mg/kg of hydrocortisone over 10 days. We can finally see the results of a trial without the complicating prophylactic indomethacin trials interfering with results. Surprisingly this study was also stopped early (a curse of such trials?!) due to financial reasons this time. Prior to stoppage though they managed to recruit 255 to hydrocortisone and 266 to control groups. All infants in this study were started on hydrocortisone within 24 hours of age and the primary outcome in this case was survival without BPD at 36 weeks of age.
All infants were less than 28 weeks at birth and therefore had a high risk of the combined outcome and despite the study being stopped early there was indeed a better outcome rate in the hydrocortisone group (60% vs 51%). Another way of looking at this is that to gain one more patient who survived without BPD you needed to treat 12 which is not bad at all. What is additionally interesting are some of the findings in the secondary analyses.
The lack of a difference in males may well reflect the biologic disadvantage that us males face overcoming any benefit from the hydrocortisone. In fact for the females studied the number needed to treat improves to 6 patients only! Short term outcomes of less ventilation are sure to please everyone especially parents. Lastly, a reduction in PDA ligation is most probably related to an antiprostaglandin effect of steroids and should be cause for joy all around. Lastly, a tip of the hat to Dr. Watterberg is in order as those infants who were exposed to chorioamnionitis once again show that this is where the real benefit may be.
But what about side effects?
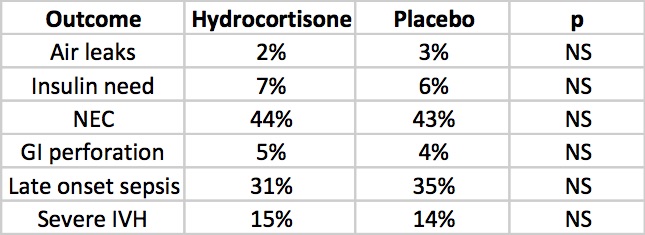
The rate of NEC is quite high but is so for both groups but otherwise there is nothing much here to worry the reader. Once and for all we also see that by excluding concurrent treatment with indomethacin or ibuprofen the rate of GI perforation is no different this time around. Reassuring results indeed, but alas the big side effect, the one that would tip the scale towards us using or abandoning treatment has yet to be presented. Steroids no doubt can do great things but given the scare from 2001 we will need to see how this cohort of babies fares in the long run.
The follow-up is planned for these infants and the authors have done an incredible job of recruiting enough patients to make the results likely believable. I for one can’t wait to see what the future holds. If I was a betting man though I would say this ultra low dose of hydrocortisone may be just the thing to bring this therapy finally into the toolbox of neonatal units worldwide. We have been looking for the next big thing to help improve outcomes and good old hydrocortisone may be just what the doctor ordered.
What a hard topic to resist commenting on. This was all over twitter and the general media this week after the New England Journal published the following paper; Antenatal Betamethasone for Women at Risk for Late Preterm Delivery. The fact that it is the NEJM publishing such a paper in and of itself suggests this is a top notch study…or does it?
Is there a benefit to giving antenatal steroids from 34 0/7 – 36 5/7 weeks?
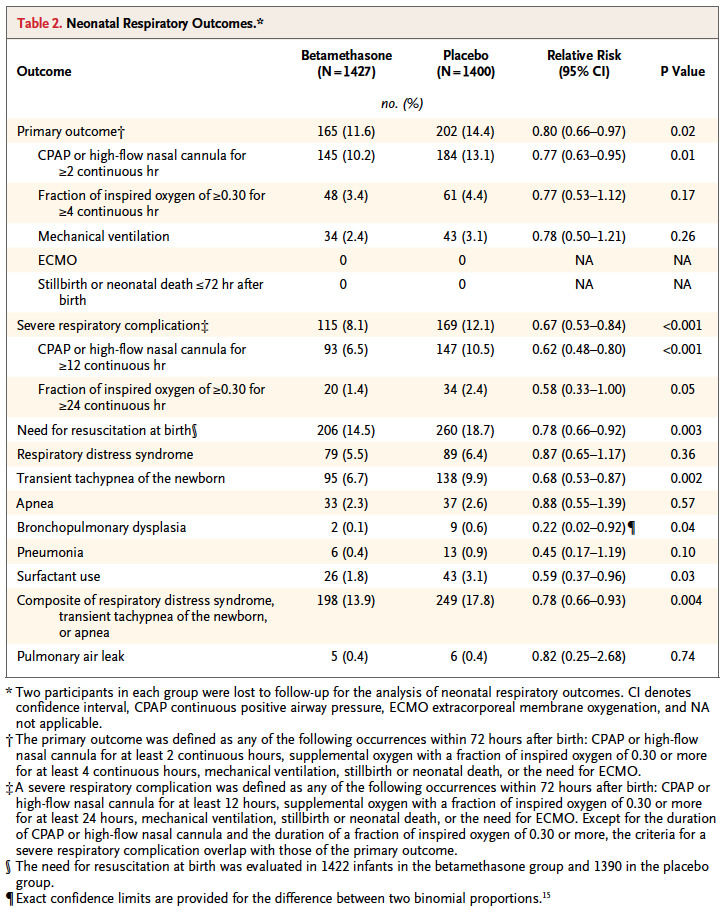
That is the central question the authors here sought to answer. Would women who had a high risk of delivering during this time period have less risk of a composite primary outcome of treatment in the first 72 hours (the use of continuous positive airway pressure or high-flow nasal cannula for at least 2 hours, supplemental oxygen with a fraction of inspired oxygen of at least 0.30 for at least 4 hours, extracorporeal membrane oxygenation, or mechanical ventilation) or stillbirth or neonatal death within 72 hours after delivery.
On the surface this seems like a very worthwhile set of outcomes to look at and the authors found in the end some pretty remarkable findings in a total of 2827 women randomized to placebo or betamethasone.
Looking at the results one sees that the primary outcome showed a significant difference with 2.8% less infants experiencing these conditions. However, when one looks at the details the only contributor to this difference was the need for CPAP or HFNC for >= 2 hours. A need for over 30% FiO2 for > 4 hours was also not different. No differences were noted in mechanical ventilation, ECMO, deaths whether stillbirths or neonatal deaths. Curiously, significant differences for secondary outcomes were seen with incidence of severe respiratory distress, and need for CPAP for over 12 hours.
These results are not truly that surprising at least for the primary outcome as if you asked most people working in the field of Neonatology how likely death, need for ECMO or even mechanical ventilation are from 34 – 36 weeks they would tell you not very likely. The other thing to consider is that the only real significant difference was noted for infants needing CPAP or HFNC for at least 2 hours. While this would interrupt maternal infant bonding, it wouldn’t necessarily mean an admission but rather in some cases observation and then transfer to the mother’s room.
Is it worth it?
To answer this question you need to know the best and worst case scenarios I suppose. Based on the reduction of 2.8%, you would need to treat 35 women with betamethasone to avoid the primary outcome but of course there is a range based on the confidence intervals around this estimate. The true estimate lies somewhere between 18 – 259 to avoid the outcome. Having said that, the estimate to avoid severe distress is 25 patients with a range of 16 – 56 which is pretty good value. In a perfect world I would probably suggest to women that there seems to be a benefit especially if one notes that in this study only 60% of the women received 2 dose of betamethasone so if rates of administration were higher one might expect and even better outcome. Ah but the world is not perfect….
There is only so much betamethasone to go around.
I find it ironic but the same day that this article came across my newsfeed so did a warning that we were about to run out of betamethasone vials in a certain concentration and would need to resort to another manufacturer but that supply may also run out soon as well. The instructions were to conserve this supply in the hospital for pregnant women.
In Canada as reported by the Canadian Neonatal Network in 2010, 38.1% of babies admitted to NICUs were below 34 weeks. Given that all babies would be admitted to NICUs at this gestational age and below that likely represents the percentage of births in those ages. An additional 31.8% or almost an equal number of babies will be born between 34 0/7 to 37 0/7 weeks meaning that if we were to start treating women who were deemed to be at risk of preterm delivery in that age range we would have a lot of potential women to choose from as these are the exact women in this strata who actually delivered early in Canada.
If I am forced to choose whether to give betamethasone to the mothers under 34 weeks or above when the resource we need is in scarce supply I don’t think there is much choice at all. Yes, this article comes from a reputable journal and yes there are some differences some of which are highly significant to consider but at least at this time my suggestion is to save the supply we have the babies who will benefit the most.
The scenario is often the same. Faced with a child born to a mother with risk factors for sepsis you decide to start antibiotics. The time comes closer to 36 – 48 hours when you must decide whether or not to continue. Each time we examine our results and look at cultures and try to do what is right. Yet defining right is sometimes hard for so many. If we had 100% sensitivity and specificity for all our tests it would be easy but we don’t. So what can we do?
If I had to have one wish though it would be that we could improve upon our diagnostic accuracy when it comes to treating suspected infections in the newborn. As health care providers we have an extremely loud inner voice trying to tell us to minimize risk when it comes to missing a true bacterial infection. On the other hand so much evidence has come forth in the last few years demonstrating that prolonging antibiotics beyond 48 hours is not just unwise in the absence of true infection but can be dangerous. Increased rates of necrotizing enterocolitis is just one such example but other concerns due to interfering with the newborn microbiome have arisen in more recent years. What follows are some general thoughts on septic workups that may help you (and myself in my own practice) as we move ahead into the New Year and may we cause less harm if we consider these.
The Role of Paired Blood Cultures
Although not published by our centre yet, we adopted this strategy for late onset sepsis a couple years back and have seen a significant reduction in work-ups deemed as true infections since adoption. While the temptation to do only one blood culture is strong as we have a desire to minimize skin breaks consider how many more there will be if you do one culture and get a CONS organism back. There will be several IV starts, perhaps a central line, repeat cultures etc. If you had done two at the start and one was positive and the other negative you could avoid the whole mess as it was a contaminant from the start. On my list of do no harms I think this may have the greatest benefit.
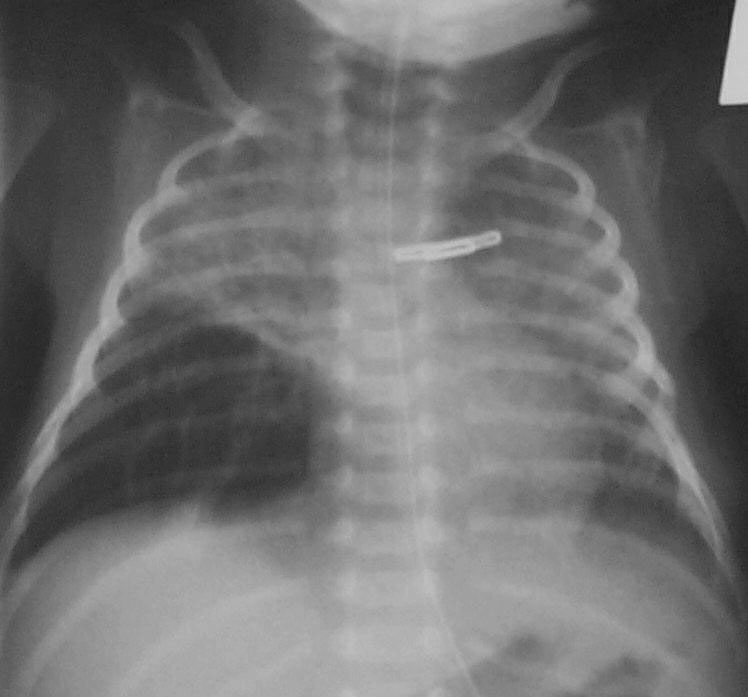
The Chest X-Ray Can Be Your Friend
While I am not a fan of routine chest x-rays I do believe that if you are prepared to diagnose an opacification on a chest x-ray as being due to a pneumonia (VAP or in those non-ventilated) that you need to follow this up with a repeat x-ray 24 – 48 hours later. If the opacity is gone it was atelectasis as a true pneumonia will not clear that easily. Well worth the radiation exposure I say.
If You Are Going To Do a Work-up Make It A Complete One
We hear often in rounds the morning after a septic work-up that the baby was too sick to have an LP and that we can just check the CSF if the blood is positive. There are two significant problems to this approach. The first which is a significant concern is that in a recent study of patients with GBS meningitis, 20% of those who had GBS in the CSF had a negative blood culture. Think about that one clearly… relying on a positive culture to decide to continue antibiotics may lead to partially treated GBS meningitis when you discontinue the antibiotics prematurely. Not a good thing. The second issue is that infants with true meningitis can have relatively low CSF WBC counts and may drift lower with treatment. Garges et al in a review of 95 neonates with true meninigits found that CSF WBC counts >21 cells per mm3 had a sensitivity of 79% and specificity at 81%. This means that in those with true meningitis 19% of the time the WBC counts would be below 21 leading to the false impression that the CSF was “fine”. If antibiotics were effective it could well be by 48 hours that the negative CSF culture you find would incorrectly lead you to stop antibiotics. Message: Do the CSF sampling at the time of the septic work-up whenever possible.
If We Aren’t Prepared To Do a Supra Pubic Aspirate Should We Not Collect Urine At All?
This provocative question was asked by a colleague last week and is based on the results of a study which was the topic of the following post: Bladder Catherterizations for UTI: Causing more harm than good? The gist of it is that it would appear that in many cases the results of a catheter obtained urine cannot be trusted. If that is the case then are we ultimately treating infections that don’t actually exist when the only positive culture is from a urine. I believe using point of care ultrasound to obtain specimens from a SPA will be the way to go but in the meantime how do we address the question of whether a UTI is present or not? May need to rely on markers of inflammation such as a CRP or procalcitonin but that is not 100% sensitive or specific either but may be the best we have at the moment to determine how to interpret such situations.
Lastly, Slow Down And Practice Good Hand Hygiene
So much of what I said above is important when determining if an infection is present or not. The importance of preventing infection cannot be understated. Audits of hand hygiene practice more often than not demonstrate that physicians are a group with some of the lowest rates of compliance. Why is that? As a physician I think it has nothing to do with ignorance about how to properly perform the procedure but rather a tendency to rush from patient to patient in order to get all the things done that one needs to do well on service or call. If we all just slow down a little we may eventually have less need to run from patient to patient as the rate of infections may drop and with it demand for our time.
If slowing down is something that you too think is a good idea you may want to have a look at the book In Praise of Slowness by Carl Honore (TED Talk by Carl Below) which may offer some guidance how to do something that is more easily said than done. Here is hoping for a little slower pace in the new year. We could reap some fairly large benefits!
I will admit it. I resist change at times just like many others. This may come as a surprise to some of you who have worked with me and accused me of bringing too much change at times to the units. The truth though is that when one understands something and is enthusiastic about implementation the change does not seem so difficult. When it isn’t your idea though we may find ourselves a little uneasy about adopting this unfamiliar practice.
Such has been my experience with nasal HFOV. It is a strategy that has been around for over five years but has seen slow adoption among centres in Canada and has trickled into practice in Winnipeg on a few occasions. In each occasion when I have been asked about either continuing or perhaps starting this therapy I have shrugged my shoulders and confessed my inexperience with the modality. Sure I have used HFOV through an ETT but through prongs or a mask?! How would it work? Could it cause harm? What would the actual indications be? How would our in house physicians and NNPs respond to abnormal gases overnight even if I felt comfortable with using it? These sorts of questions have led to virtual inertia in my acceptance of the strategy.
Before I go on it would be good to see an example of how it is set up. The MedinCNO device is capable of delivering such non-invasive HFOV and can be seen in this short video.
One could use the strategy either prophylactically to extubate an infant or as rescue to prevent reintubation if trials of either CPAP or NIPPV were unsuccessful. HFOV is known to be very effective at clearing CO2 when used through an ETT so perhaps nasal application could also lower pCO2 and achieve a similar effect. This was tested using a neonatal lung simulator by Mukeji A et al Nasal high-frequency oscillation for lung carbon dioxide clearance in the newborn. In this study CO2 was introduced into the manequin and the amount of exhaled CO2 determined while on CPAP, NIPPV and nasal HFOV. Interestingly during CPAP no exhaled CO2 could be detected while CO2 clearance occurred during NIPPV and nasal HFOV although it was three-fold greater with HFOV. In theory then CO2 clearance would appear to be better so in the case of ventilatory failure as evidenced by CO2 retention this modality would seem to win out.
Clinical Evidence for Use
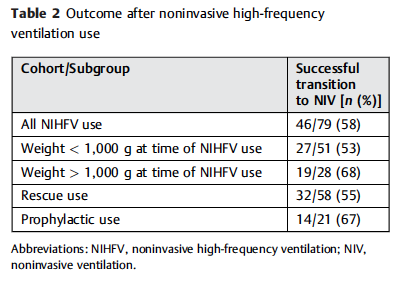
There is one RCT in term infants with TTN to support the practice while the rest are unblinded case series with no controls. Four Canadian NICUs recently described their experience however using a retrospective analysis. Included were 79 instances of HFOV distributed as follows; 73% utilized as rescue from another mode and in 27% used as the primary mode for extubation. The outcomes are shown in the table:
In 45% of cases the patients needed intubation after first trialing CPAP or NIPPV while in 33% of cases following extubation the infants needed replacement of the endotracheal tube. The numbers here are small so it is difficult to truly compare them to other studies with confidence but reintubation rates of 40-44% have been noted recently when using NIPPV or CPAP so the numbers are at least consistent.
One aspect though that caught my eye was the duration of use for HFOV across these 79 patients. The median use was 57 hours with the longest duration being just over 400 hours. It would seem that the use of this modality for the most part is as a bridge to something else. The median duration of 2.5 days is much shorter than the weeks that some of our smallest infants remain on CPAP/NIPPV for. Whether for rescue or prophylaxis this is not a long term option.
Another point worth noting though is the question of whether it is the pressure or oscillatory wave that is leading to success. As the authors note, there were a wide range in applications of MAP, delta P and frequency.
MAP ranges from 8 – 24 cm H2O while frequency from 6 – 14 hz and amplitude varied widely depending on the device used but was as high as 100%. While high MAP has been used invasively though an ETT I can’t help but wonder if in some cases the real benefit was the high MAP. What would happen for example if the centres had simply raised the CPAP to 10, 12 or even higher?
In the end it would seem that in principal it is an effective therapy that may be able to remove CO2 more efficiently than the other modes. What we don’t have are RCTs in the smallest babies comparing HFOV to NIPPV or CPAP with adequate power to detect differences. I suspect these will come soon enough but what do we do in the meantime? The main reservation I have has to do with safety. We truly have little if any data on this without proper trials to ease such worry. When a patient is in front of us though and is failing CPAP or NIPPV what are we to do? Should we intubate or trial this modality based on the evidence thus far?
I might be tempted to trial HFOV in this circumstance but as with any new therapy we need education for all staff. Everyone caring for our infants need to understand what they are using and how to respond based on clinical findings. This is the real issue with safety that I see and until such time that we have widespread education across RRT, nursing and medicine I would suggest we use this with trepidation. This is not a rejection of the modality in the least but rather a call to come together as a team and see how implement this in such a way that will provide direction to caregivers, provide a consistent approach with respect to length of use, indications and when to change direction entirely. Time to call a meeting of the minds I think.
It is one of the first things that a medical student pledges to do; that is to do no harm. We are a fearful lot, wanting to do what is best for our patients while minimizing any pain and suffering along the way. This is an admirable goal and one which I would hope all practitioners would strive to excel at. There are times however when we can inadvertently cause more harm than good when we try to avoid what we perceive is the greater harm.
This is the case when it comes to collecting a sample of urine for culture as part of a full septic workup. If you ask most healthcare providers they will freely acknowledge that the gold standard for determining whether an infant has a UTI is a supra pubic aspirate (SPA). We so rarely do them these days however due to a whole host of reasons. Problems with collection include the timing and accuracy of needle placement both of which may often lead to an empty tap. Secondly after a number of missed attempts and a crying infant who appears to be in pain it is understandable why bedside nurses may become frustrated with the entire experience and urge the person performing such procedures to settle on a bladder catheterization (BC) to obtain the specimen.
All in all the BC performed quite poorly when compared to the gold standard. The false positive rate compared to SPA was 71.1%! That is to say that only 28.9% of SPA samples were positive compared to BC. Similarly urinalysis sensitivity and specificity from BC were 66.7% (95% CI, 44.68% to 84.33%) and 93.22% (95% CI, 83.53% to 98.08%), respectively. This means that only 2/3 of the time was the urinalysis abnormal on a BC in the presence of a true UTI. Somewhat reassuring is that when there really was no UTI the urinalysis was mostly negative but in almost 1/10 patients it would not by itself rule out a UTI.
What Is The Harm in Continuing BC Instead of SPA?
When we try to avoid the perceived painful experience of a SPA we are going to wind up treating a large number of patients for a presumed UTI who don’t have one. The harm in this is the exposure of such infants to prolonged courses of antibiotics which has been a subject discussed many times over on this site. We put our patients at risk of antibiotic resistance and shifts in the gut microbiome which in the case of the preterm infant puts them at risk of necrotizing enterocolitis. There are many other concerns with prolonging antibiotics but these few should be reason enough to strive for accuracy in obtaining the right specimen in the right way. Putting it in a slightly different perspective, would you settle for an alternative test to a lumbar puncture which claimed to miss 1 in 10 cases and also found meningitis where there was none 71.1% of the time?!
A Way Forward – A Recipe For Success
As the saying goes, measure twice and cut once. With the use of bedside ultrasound there should be no need to guess as to whether the bladder is full or not. Secondly the placement of the needle should no longer need to rely on landmarking but actually seeing where the best place for needle placement is. Assessing the bladder by ultrasound is easy and is already employed at the bedside by nurses in many areas of the hospital. There should no longer be a reason for the empty tap as the practitioner can be called when the baby is ready as evidenced by a good amount of urine in the bladder.
Given that we have some time to do the blood culture and LP, while we wait for the SPA to be done either sucrose in the premature infant or IV analgesic may be given for the SPA while in the term or older infant there is an opportunity to put a topical analgesic cream over the site. There really is little need for pain to factor into this any longer.
Ask any health care provider and they will tell you they want to do the best they can for their patient. This study shows us that performing a BC is failing to meet that goal. We need to change our ways and return to the practice of the SPA but this time we have to get it right.
As I read through the new NRP recommendations and began posting interesting points on my Facebook Page I came across a section which has left me a little uneasy. With respect to a newborn 36 weeks and above who is born asystolic and by ten minutes of age continues to remain so and has an apgar score of zero the recommendation that has been put forward is this:
An Apgar score of 0 at 10 minutes is a strong predictor of mortality and morbidity in late-preterm and term infants. We suggest that, in babies with an Apgar score of 0 after 10 minutes of resuscitation, if the heart rate remains undetectable, it may be reasonable to stop resuscitation; however, the decision to continue or discontinue resuscitative efforts should be individualized. Variables to be considered may include whether the resuscitation was considered to be optimal, availability of advanced neonatal care, such as therapeutic hypothermia, specific circumstances before delivery (eg, known timing of the insult), and wishes expressed by the family (weak recommendation, very-low-quality evidence).
There are some significant problems with this part of the statement.
They claim that the apgar score at ten minutes is a strong predictor but when you look at the analysis of the evidence presented in the body of the paper it is weak at best. I am not clear how one declares the prediction is strong in the face of poor evidence but I will acknowledge intuitively that this makes some sense but do challenge them on the use of the word “strong”.
2. They are correct in acknowledging that the introduction of hypothermia in such settings has changed the landscape in as much as I find it quite difficult to prognosticate unless a child is truly moribund after resuscitation. Given such uncertainty it is concerning to me that this recommendation may be committed to memory incorrectly in some places that do have access to cooling and may be used more rigidly as though shalt stop at 10 minutes.
3. In the middle of a resuscitation it is quite difficult to process all of the facts pertaining to a particular newborn while orders for chest compressions, emergency UVCs and epinephrine are being given. Can we really individualize within ten minutes accurately and take the families wishes truly into account? This just does not seem practical.
4. The families wishes are taken into account but inserted as a “weak recommendation”. How can the wishes of the family in any family centred model of care be minimized in such a way even if we believe the situation to be dire?
5. Since the introduction of hypothermia there appears to be a near 50% survival rate in such newborns and as the authors state 27% of survivors who received cooling had no moderate or severe disability. Here in lies my greatest issue with this guideline and that is the hypocrisy this position takes when you compare populations at 23 and 24 weeks gestational age. Survival at these GA in the recent NEJM study of almost 5000 preterm infants under 27 weeks were 33 and 57 % respectively at 23 & 24 weeks with rates of survival without moderate or severe disability being 16 and 31% in the two groups. The fallout from this and other studies at the extremes of gestational age have been that we should be more aggressive as the outcomes are not as bad as one would predict. How can we argue this for the 23-24 week infants and for term infant with the same likelihood of outcomes we would unilaterally stop in many centres?!
So Now What Do We Do?
We are supposed to be practising family centred care and much like the argument at the edge of viability the same should apply here. The wishes of the family should never be minimized. Arguably it may be very difficult in such an unexpected scenario to appraise a family of the situation and have clarity around the issue but if a heart rate can be restored after a few more minutes do we not owe it to the family and the child to bring the infant back to the NICU and see what transpires especially if cooling is available?
The million dollar question of course is where do we draw the line? No heart rate at 15, 20 minutes? Based on the evidence thus far it seems to me that a little longer than 10 minutes is reasonable especially in well equipped centres with access to cooling and modern ventilation and treatments for pulmonary hypertension. How long though must be individualized and should be determined in partnership with the team caring for the patient which must include the family.


 Like any scare though, with time fear subsides and people begin asking questions such as; was it the type of steroid, the dose, the duration or the type of patient that put the child at risk of adverse development? Moreover, when death from respiratory failure is the competing outcome it became difficult to look a parent in the eye when their child was dying and say “no there is nothing more we can do” when steroids were still out there.
Like any scare though, with time fear subsides and people begin asking questions such as; was it the type of steroid, the dose, the duration or the type of patient that put the child at risk of adverse development? Moreover, when death from respiratory failure is the competing outcome it became difficult to look a parent in the eye when their child was dying and say “no there is nothing more we can do” when steroids were still out there.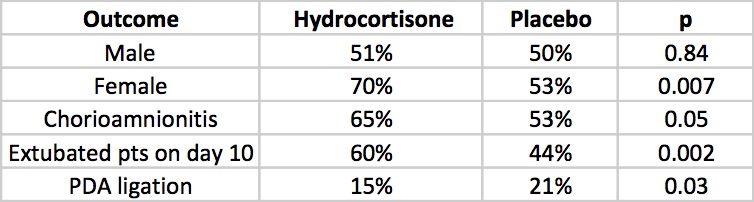


 If the opacity is gone it was atelectasis as a true pneumonia will not clear that easily. Well worth the radiation exposure I say.
If the opacity is gone it was atelectasis as a true pneumonia will not clear that easily. Well worth the radiation exposure I say.