Another year has passed and another World Prematurity Day is upon us. I thought about what to write for this day that draws attention to premature infants worldwide and was hit with many ideas which no doubt will form the basis for many posts to come. There was one thought that struck me though as being so important to think about as we push forward, striving to improve survival across the globe for our smallest patients. There is no doubt that you will have heard the expression “just because we can do something, should we?” In 2015 I don’t think this applies more than at this very moment.
At a Tipping Point
You see we are at a tipping point as Malcolm Gladwell explained so brilliantly in his book by the same name. In April of 2015 Rysavy et al published the results of survival and morbidity data for infants born in 24 US hospitals between the ages of 22 – 26 weeks. The nearly 5000 infants included demonstrated two very important things. Firstly, survival is possible at 22 and 23 weeks and there is a chance, albeit less than 50% that these infants will survive without moderate or severe disability. Secondly, at these gestational ages 75% of hospitals included provided active resuscitation to these infants. Given that this is the largest study out there and shows that survival is possible and we can expect to see some good outcomes it would seem logical to move forward with universal resuscitation of these infants would it not?
You Are Going To Practice on What?!
As the saying goes though, “Perfect Practice Makes Perfect”. Not all hospitals have equal performance at these gestational ages which is demonstrated in the ranges of outcomes across hospitals as shown in the Rysavy paper. To even suggest that we need to practice on premature babies will no doubt leave many of you feeling queasy but in essence that is what is truly needed to improve our outcomes further. An infant born at 22 – 24 weeks is vastly different than one born at a later gestational age. Their skin is extremely fragile and prone to breakage with resultant risk of infection. Their lungs are in a stage of development that has yet to produce any real abundance of gas exchanging alveoli and their brains lacking the sulci and gyri that are to come many weeks later. They are in need of meticulous “best practice” care and without that their outcomes are certainly to be influenced. Depending on the centre though, you may see 5, 10, 15, 20 patients a year at these ages. How can a team possibly gain enough experience in treating these children appropriately if they see 1 or 2 every two months? Add to this that you may have 10 different Neonatologists so on average each of you may take care of one patient a year at birth. This is a recipe prone to poor outcomes if you ask me.
The Evolution of the Small Baby Unit
The answer no doubt will lie in creating smaller teams; so called “Small Baby Units”. Such units have small groups of health care providers dedicated to treating such infants thereby increasing the frequency of individuals exposure to these babies. There is some recent evidence published in Pediatrics that supports this notion. Small Baby Unit Improves Quality and Outcomes in Extremely Low Birth Weight Infants. In this study a period of two years before and four years after opening such a unit were compared across a number of measures. The findings were as follows “There was a reduction in chronic lung disease from 47.5% to 35.4% (P = .097). The rate of hospital-acquired infection decreased from 39.3% to 19.4% (P < .001). Infants being discharged with growth restriction (combined weight and head circumference <10th percentile) decreased from 62.3% to 37.3% (P = .001). Reduced resource utilization was demonstrated as the mean number per patient of laboratory tests decreased from 224 to 82 (P < .001) and radiographs decreased from 45 to 22 (P < .001).” I hope you would agree that achievements such as these are worth the effort to create such an environment. Future studies I believe will confirm these findings although having the gold standard RCT may be difficult to achieve as I suspect we will have lost equipoise.
This brings me to the final point though and that is whether we are ready as a health care system for the increase patient load that this change will bring about. Based on an expected stay of 4 months for a baby born at this age and knowing the average number of such babies delivered per year, we would be looking at about 600 patient days per year added to each hospital’s occupancy in our two centres. This represents about a 5% increase in patient bed days per year. Five percent may not seem like a large increase at first blush but when we like many hospitals have been trying to deal with staffing issues and many days in which we are at or near capacity, this is not an insignificant challenge. It is a challenge though that we must face head on. Resources must be found, and space provided to accommodate for these children. We live in a world now where it is not solely up to us but to the family as well who must be integral to any such decision to either pursue or withdraw care. News of such infants surviving has spread to the public and I have no doubt that many families will have heard stories of such survivors. The next phase of care for these infants must address the shortcomings in care at the moment.
How do we educate families about what to expect in the long run?
How do we support these families when they make such difficult decisions either way?
How do we support our front line staff who may hold quite discrepant viewpoints about what is “right” yet expect them to function as one team moving clearly in a direction that supports the family?
How do we ensure that our focus on our smallest infants does not distract us from the attention needed by those born at later gestational ages?
I could go on but these are just some of the questions that I hope the next year begins to tackle. We are in the midst of an evolutionary point in Neonatology and we owe it to ourselves and the families we care for to navigate this change as best we can.
In 2018 where do we stand on this question? Upcoming retrospective trials and work by EPIQ-4 may help to resolve this issue. In the meantime what does the existing evidence say?
The decision to extubate an extremely low birthweight infant is one of the most common sources of disagreement and anxiety in the NICU. As a resident, I recall an unwritten rule that “no baby under 750g will have a trial of extubation as they will most certainly fail”. As time went on however, studies suggested that not only is this a false statement but also that the duration of intubation was directly correlated with risk of BPD. As Danan described, for infants less than a 1000g, delaying extubation when they had reached minimal settings did not result in lower rates of BPD. Moreover 60 – 70% of infants who have such extubation attempts are not reintubated within a week, so it is possible to have success.
The detractors however express concern about the 30-40% who do require reintubation and worry that harm will be caused by such acts. Frequent concerns are voiced with respect to potential trauma to the airway leading to subglottic stenosis; potentially increasing the risk of BPD and finally the belief that attempts are futile so why put parents through the stress in the midst of perceived near certain failure. The problem with these perceptions however is that they are mostly the culmination of confirmation bias. Patients that have multiple failed extubations are remembered especially when they develop significant complications, while the ones who extubate successfully are quickly forgotten. This is not intentional in any way but simply a human tendency to follow the pattern of “the squeaky wheel getting the grease”. The preemies who do poorly are front and centre as they take up a great deal of our time & attention while the ones who do very well while celebrated, are not as easily remembered for the success they demonstrated when extubated.
Being someone who believes in extubating as soon as possible though I was surprised several months ago to find a paucity of data demonstrating that there was in fact support for the practice in terms of better outcomes being associated with early extubation. While small studies certainly pointed in that direction the real question was about to be answered in the study that follows.
Is it better to fail multiple times or be intubated once for the duration of ventilation.
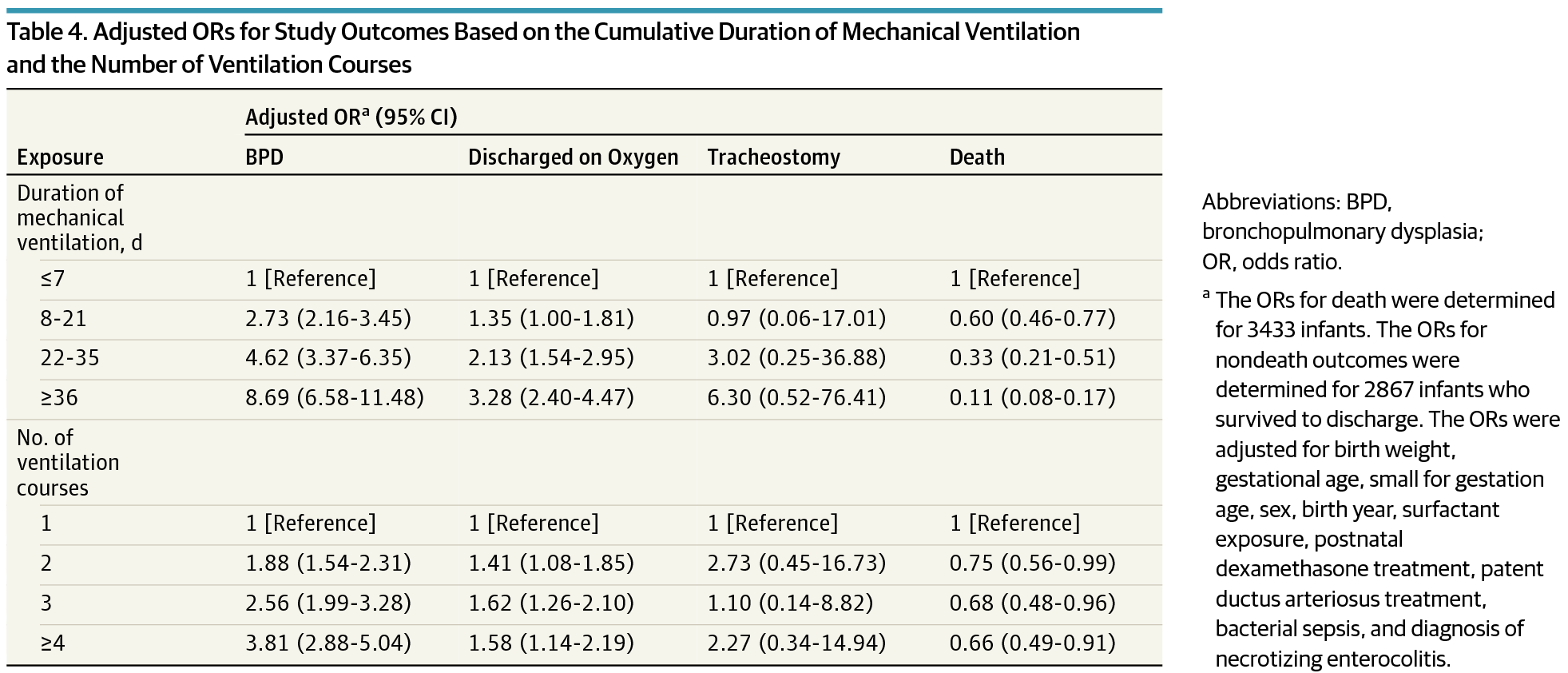
This is the central question that I believe has been answered as good as it will ever be by EA Jensen et al in JAMA this past month “Effects of Multiple Ventilation Courses and Duration of Mechanical Ventilation on Respiratory Outcomes in Extremely Low-Birth-Weight Infants.” This retrospective review included 3343 infants below 1000g and examined the primary outcome of BPD and secondary outcomes of death, continued supplemental oxygen use at the time of discharge, and tracheostomy among survivors. As you might expect, regardless of whether one compared duration of ventilation or number of reintubations, variables such as need for surfactant, postnatal dexamethasone, PDA treatment and NEC became more common as exposure to either outcome increased. When a logistic regression model was applied though it became evident that the odds ratio for BPD increased to a much greater degree with increasing duration of ventilation than the number of attempts.
To quote the authors:
“After adjustment for the cumulative duration of mechanical ventilation, a greater number of ventilation courses was not associated with an increase in the risk-adjusted odds of supplemental oxygen use at discharge. The number of ventilation courses remained associated with increased risk of BPD only among infants exposed to 4 or more courses.”
The Needs of The Many Outweigh The Needs of The Few
In other words, for an infant to have an increased risk of BPD they would need to have failed extubation four or more times! It is not easy to predict with certainty who these children will be but if we take these findings as accurate (since I believe we will not see an RCT of this magnitude anytime soon) is it ethical to keep a child intubated due to the belief that they might fail? On the contrary, how can we not try when failure is not associated with adverse outcome? In fact none of the secondary outcomes were found to be increased either. Importantly, there was no difference in the need for a tracheostomy in this population which may serve as a proxy for lack significant airway injury from multiple intubations. The goal of this post is to provide all of us who care for these preemies with the reassurance that if they fail extubation, once, twice and even three times that is still a good thing. For the ones that fail more than that, if only we had a crystal ball we might have spared them that risk but given that we live in a world without this ability, we owe it to our patients to try. Moreover, we owe it to the parents of these children to educate them that failure can still be a good thing.
May I never have a near 100% success at extubating my patients on the first try. If I truly care for them I will embrace my failures and know that I have done the right thing.
The 10th Annual Bowman Symposium did not disappoint! World class presenters gathered to provide a top to bottom update on a variety of topics spanning from the nervous system to Genetics. After a day and a half of presentations though I was left with some concerning (scary) thoughts and it seemed Halloween was the perfect time to share them with you!
How Much Oxygen is Just Right?
Dr. Ola Saugstad provided a wonderful history of the use of oxygen in Neonatology. After his talk it was clear that oxygen is most definitely a drug with its most concerning side effect being the production of oxygen free radicals in the body. If we are too restrictive aiming for saturations of 85 – 89% we spare our infants ROP but put them at greater risk of death. Too high at 91 – 95% and they may survive but with more ROP (BOOST and SUPPORT). If we resuscitate with 100% oxygen that is associated with worse outcomes but so too is 21% in our newborns < 28 weeks. The NRP would advise us to use 21 – 30% to start in this group for resuscitating but he recommends 30%. Certainly the recent publication by Jack Rabi out of Calgary suggests room air may in fact be harmful in this group as a starting point! After 50 years of research we still don’t know what to give newborns to help them start their life outside the womb. Scary.
It’s All In The Name
Next up is Dr. Aviva Goldberg who raised a very important point that I had not considered before. In every researchers quest to come up with a catchy name for their study that people will remember, the connotation is equally important. The SUPPORT study came under heavy fire (commentary here) after a surprising increase in mortality was found in the arm randomized to 85 – 89% saturations. Families sued the investigators and in their complaints they were angry about being misled. How could a study that was named the SUPPORT study do anything other than help their children? The title in and of itself they argued misled them as they never would have thought increased mortality could be a risk. Researchers make sure you test out your clever names with parents before finalizing your studies. The decision otherwise could come back to haunt you…
Jury Still Out on Bevicizumab (Avastin) for ROP
Dr. Ian Clark provided an overvue of the current state of thinking on treating ROP. For central disease in Zone 1 Avastin is preferred but for more peripheral disease laser seems to still be recommended due to its decisiveness in eliminating the disease without affecting future vision. Concerns continue though with respect to potential systemic effects of putting an anti-VEGF medication in the eye. Can it leak out and cause disruption to angiogenesis in other organs and in particular the brain? A recent poster at the CPS meeting in Toronto entitled Neurodevelopmental outcomes of extremely preterm infants treated with bevacizumab for severe retinopathy of prematurity indicates that there may be greater impairment in those receiving injections. There are several flaws in this paper though including greater numbers of males (we always do worse), more sepsis and worse SNAP-II scores in the injection group but the results have been making it into discussions leaving Ophthalmologists wondering if they are doing the right thing…very scary.
Cow’s Milk Human Milk Fortifier Is Safe For Premature Infants… Or is it?
Next up was Dr. Bill Diehl Jones who presented in vitro data on the effect of these supplements with respect to their contribution to oxidative stress. Such stress has been associated with BPD, NEC and ROP to name a few disorders in preemies. A paper published this week in which intestinal cells were exposed to human milk with HMF experienced significantly increased intracellular oxidation, cell damage, and cell death compared to those exposed to just breast milk. A paper from 2013 indicates that premature infants fed HMF experience increasing levels of urinary isoprostanes (a measure of oxidative stress). We know that infants receiving these products experience better growth and bone density than those without exposure but is there a cost? Will further research in this area drive us towards exclusive human milk based diets? The seed that has been planted in my head now questioning the safety of this product I use every day…a little frightening.
Curtailing Antibiotic Use And The Coming Black Swan
John Baier spoke about practice variation between Neonatologists in terms of the decision to prolong antibiotics or not in the face of negative cultures. While we do have variation, the good news is that we overall have cut down our tendency to prolong past 48 hours in the face of negative cultures. If we practice long enough though, the Black Swan will eventually rear its ugly head. The Black Swan is an exceptionally unusual event but one that has dramatic impact. How will we respond when a patient becomes septic after 48 hours and the antibiotics were stopped? Will we panic and change our practice entirely to avoid the internal pain again of feeling like we made a mistake or remember that we have saved countless infants from the long-term effects of indiscriminate use such as NEC, atopic disease and obesity in childhood just to name a few. It is this nagging doubt I have about how we will react that gives me cause to worry!
Finishing With a Miracle
It doesn’t seem right to end on a down note so I thought it would be worth celebrating that a cure has been found for something very scary. Hypophosphatasia is a rare disorder of the bone which was previously lethal in many cases. Thanks to research that our own Dr. Cheryl Greenberg led here in Canada we are able to successfully treat these children now. The Bowman symposium showed us incredible videos of such treated children and to end this post I found this video from Youtube of Gideon who was one of these patients treated with FDA Okays Asfotase Alfa (Strensiq). If you would like to leave this post with a smile on your face until next Halloween have a look at the video!
On occasion two articles will be published in short succession and have discrepant findings. This appears to be one of those times. Hishikawa K in Japan published a paper in September entitled Pulmonary air leak associated with CPAP at term birth resuscitation while Calebi MY from Turkey published Impact of Prophylactic Continuous Positive Airway Pressure on Transient Tachypnea of the Newborn and Neonatal Intensive Care Admission in Newborns Delivered by Elective Cesarean Section in August of this year.
The findings as we will discuss were quite discrepant which on the surface leaves the practitioner in a quandry. How do I best treat my patients? The key difference between the two studies was the finding of an increased rate of pneumothorax in the study by Hishikawa when CPAP was used in term infants with respiratory distress after delivery. Curiously prophylactic CPAP of +5 was used in both studies but the populations under study were quite different. The study by Calebi targeted infants between 34 0/7 weeks and 38/6/7 weeks vs term infants in the study from the Japanese group.
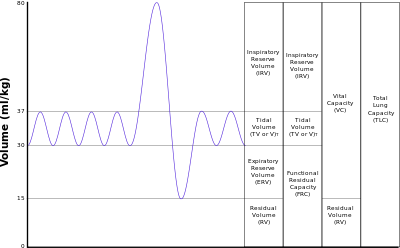
Another important difference is the utilization of CPAP which in the study by Calebi involved prophylactic administration within twenty minutes of birth and in the Japanese cohort the indication was the development of symptoms. Thinking about this for a moment, these two groups are actually quite different. A newborn with TTN has an increased amount of interstitial fluid that has not made it’s way to the hilum for reabsorption in the lymphatic system. The lungs of these infants are heavier with fluid than comparable infants without such pathology and therefore are also less compliant. Non compliant lungs are prone to microatelectasis as the infants progressively experience alveolar collapse. The longer the clinician waits to start supportive CPAP the more the lungs collapse and greater negative pressure is required to open these closing alveoli. Furthermore if there is fluid in the airway itself there is the potential for a ball valve mechanism to come into effect whereby air is able to pass through the dilated airways during inspiration but on expiration the collapse leads to air trapping. Such trapping places the infant at risk for air leak. CPAP is used to establish an adequate functional residual capacity (FRC) as indicated in this picture. Failure to do so results in atelectasis.
The Japanese study examines the impact of CPAP after a change in guidelines in 2010 suggesting that CPAP should be utilized in the delivery suite for those infants with ongoing respiratory distress. The study by Calebi really examines a different patient group being those who are near term patients with TTN who have early CPAP implemented. The early administration of CPAP may be the technique that prevents alveolar collapse as mentioned above and avoids the requirement by the infant to generate such high negative pressure with its inherent risk of air leak.
Is All CPAP The Same?
Another important distinction between the two papers is the way in which CPAP was administered. The Japanese utilized a flow inflating bag with a pressure valve and manometer while the study by Calebi employed a T-piece resuscitator. When it comes to maintaining CPAP there is no question having used both devices that I find the T-piece resuscitator much easier to use and over longer periods the reliability of the pressure delivered by the T-piece would be superior to that with the flow inflating bag. The Neopuff T-Piece Resuscitator possesses a pressure relief valve which could help during an instance when the patient is crying or breath holding. The constant flow without a relief valve could lead to airleak which is precisely the situation that may occur during the use of a flow inflating bag.
Yes there was over a three fold increase in airleak at near term gestational age in the Japanese cohort but this was not seen at all in the Turkish study in which CPAP was implemented early. So the message here is that if you start CPAP early enough you can prevent airleaks from occurring. This in and of itself is worth implementing.
Can CPAP Reduce Hospital Admission to NICU?
There is more to the story however. The Turkish group demonstrated a significant difference in admission rates to the NICU as shown in the following figure. The results here although just achieving significance should not be minimized. Avoiding progressive atelectasis decreases admission rates. The conclusion here is that there is little benefit in adopting a wait and see approach to those kids born by elective c-section. While it is true that you may be treating a significant number of healthy patients between 34 0/7 – 38 6/7 weeks with CPAP it is for a brief period and makes a significant difference in frequency of admission.
We live in an era of bed shortages and I would argue that anything we can do to reduce admissions and moreover keep babies with their parents is worth exploring. From my perspective treating these kids with the appropriate CPAP device for twenty minutes after birth is well worth it. Perhaps your unit should consider the same.
In March 2015 the CPS Infectious Diseases and Immunization Committee released a new statement entitled Preventing Ophthalmia Neonatorum. This condition otherwise known as Neonatal Conjunctivitis is potentially vision threatening and therefore is not something to be taken lightly. This statement replaces the one from 2002 and is a significant departure from the previous version. The most striking difference were the following recommendations:
Neonatal ocular prophylaxis:
Neonatal ocular prophylaxis with erythromycin, the only agent currently available in Canada for this purpose, may no longer be useful and, therefore, should not be routinely recommended.
Paediatricians and other physicians caring for newborns, along with midwives and other health care providers, should become familiar with local legal requirements concerning ocular prophylaxis.
Paediatricians and other physicians caring for newborns should advocate to rescind ocular prophylaxis regulations in jurisdictions in which this is still legally mandated.
Jurisdictions in which ocular prophylaxis is still mandated should assess their current rates of neonatal ophthalmia and consider other, more effective preventive strategies, as outlined below.
So not only are they not recommending erythromycin any longer but they ask us as health advocates to lobby to have laws changed in order to enforce such change in practice.
It has been almost half a year since this recommendation came out and what has happened in Manitoba? Nothing. I don’t believe it is inertia but rather a visceral feeling by many that this might not be the right path. In Manitoba rates of chlamydia and gonorrhea are quite high in certain pockets of the province and the reliance on people observing for signs of eye discharge after leaving the hospital is anything but certain. Large segments of the population could be put at risk of blindness or corneal damage as a minimum if we rely on all families seeking medical attention in a timely fashion. Due to circumstance that is not always possible.
This August, Dr. C. Mulholland a Pediatric Ophthalmologist in Winnipeg and Dr. Gardiner the President of the Canadian Association of Pediatric Ophthalmology and Strabismus responded to the CPS statement with their own analysis of the literature. They found the CPS statement to be not just lacking in including all the relevant evidence but in some cases actually misrepresenting research that was being quoted. I would like to commend him for critically reviewing this statement and for his analysis. A full copy of his editorial can be found here. I would encourage you to read it as it is relatively short and to the point but perhaps the best comments from his analysis are:
“Darling and McDonald conclude that, although the randomised and quasi-randomised evidence in relation to ON is not of high quality, when additional evidence is also considered, it appears that prophylaxis does reduce the risks of both GON and CON.”
“The CPS statement claims that mild irritation produced by ocular prophylaxis has been perceived by some parents as “interfering with mother–infant bonding.” This is presented as an argument for cessation of prophylaxis. This risk is overstated. The article to which the statement refers,7 in fact, found that although eye openness was lower in those infants treated with prophylaxis, “eye openness in the new-born did not significantly alter the attention of the mother toward her baby.”
The CPS statement while intending to provide solid guidance for health practitioners I believe has missed the mark. I could not agree with Dr. Mulholland more in that any attempt to change such recommendations MUST include consultation with the speciality affected by such change and that did not happen here. As a comparison, imagine the outrage if the Fetus and Newborn committee made a recommendation on the management of inguinal hernia before discharge and did not consult with Pediatric Surgeons who ultimately would be impacted by such a recommendation.
The one battleground area may be in the situation in which a mother has screened negative for GC and insists on not treating. Previously this would cause some consternation among our health care team but if we know the result is negative, they appear to be reliable and are educated about the signs to watch for this may not be a battle worth having.
While I remain a tremendous proponent of the work being done by the CPS I believe they missed the mark on this one. All statements must include a comprehensive evaluation of the literature which includes all relevant studies. Cherry picking articles to help prove ones bias does not lead to good recommendations and for that reason at least in Manitoba I do not see us changing our practice.
Nick is a tremendous advocate for premature infants and their families everywhere and as President and Co-Founder of Graham’s Foundation certainly puts himself front and centre. For more information on the incredible work he and his team are doing please see their website at and if you are in the New York area please consider attending their charity benefit to help raise some funds to continue the work that they do.
As it pertains to his question though it did get me thinking. How does a National body like the AAP determine best practice suggestions for a country with 50 states in which roughly 320 million people reside? Using 2013 USA census data ,showing 23.1% of it’s citizens are under 18 this equates to nearly 74 million children. This is a daunting task no doubt and due to regional variation in terms of expertise and available resources not all policies or guidelines are possible to implement equally or at all.
The article that is being addressed in his question of the day is from Med City News which addresses the latest statement from the AAP on managing an anticipated birth before 25 weeks. For the actual statement that the article refers to please see this link which will direct you to the actual paper.
When the Canadian Pediatric Society (CPS) reaffirmed their statement in January 2015 it drew a fair bit of criticism from Canadian Neonatologists and others from abroad due to it’s draconian approach to infants at 22 and 23 weeks gestation. In the CPS statement the following was written in the recommendations section with respect to these two gestational ages which also encompassed 24 weeks as well.
“At 22 weeks’ GA since survival is uncommon, a non-interventional approach is recommended with focus on comfort care”
“At 23 and 24 weeks’ GA active treatment is appropriate for some infants”
What drew the ire of these health care providers was the apparent limitation of resuscitation based on gestational age. It did not seem that consideration was being given to potential inaccuracies with gestational age dating which at best in the first trimester are +/- a few days and in the second trimester may be off up to 1-2 weeks. Furthermore no mention was made of accounting for other factors such as the findings on an ultrasound which if very discrepant might suggest an older fetus or perhaps equally important the wishes of the parents. What were their past experiences, religious beliefs or lengths to which they had tried for this pregnancy. The 16 year old single mother who conceived via rape might be expected to have a vastly different perspective than the mother at 43 who has tried 5 rounds of IVF and has finally conceived her first baby. Many of these points were highlighted in a response by a large group of care providers in a paper entitled “CPS position statement for prenatal counselling before a premature birth: Simple rules for complicated decisions.”
Now we have a new statement from the American Academy of Pediatrics which I have to complement as it addresses a number of concerns that the above group had with the Canadian version.
1. Fetal gestational age, as currently estimated, is an imprecise predictor of neonatal survival, but 22 weeks of gestation is generally accepted as the lower threshold of viability.
2. Although most infants delivered between 22 and 24 weeks’ gestation will die in the neonatal period or have significant long-term neurodevelopmental morbidity, outcomes in individual cases are difficult to predict.
3. Outcomes of infants delivered at 22 to 24 weeks of gestation vary significantly from center to center.
4. Because of the uncertain outcomes for infants born at 22 to 24 weeks’ gestation, it is reasonable that decision-making regarding the delivery room management be individualized and family centered, taking into account known fetal and maternal conditions and risk factors as well as parental beliefs regarding the best interest of the child.
The first four points address the issues of uncertainty in dates, variable outcomes and the importance of taking a family centred approach. On the surface this seems like the perfect statement but I have highlighted the third point as it really gets to what Nick Hall is referring to (or at least my interpretation). We know that there is a great variability in outcomes from 22-26 weeks across the US based on the recent study by Rysavy et al. In this study which involved 24 hospitals with tertiary care centres, the median survival across all hospitals at 22 weeks (who actively resuscitated infants) ranged from 0 – 14.6% and at 23 weeks 23.8 – 37.1%. Imagine you are a parent at a centre that has a zero percent survival rate at 22 weeks. Should the hospital inform you of that and if after hearing that you still want “everything done” should the Neonatal team resuscitate your infant? There is no doubt that the parental wishes as outlined in point 4 are important but I would counter that there is also little point in putting a family through a futile exercise.
Vince Lombardi the former head coach of the Green Bay Packers produced the following quote that has been used many times since his heyday in the 1960s. “Practice does not make perfect. Only perfect practice makes perfect”
This could not be more applicable to the situation in many centres thoughout the US. Resuscitating 22 and 23 week infants can be done and in a manner of speaking is a form of practice. Should centres though who have not “perfected” their approach by having rigorous audits of their practice, a “golden hour” approach and lastly the best equipment for resuscitation continue to offer families who wish to “do everything” just that? I would say no. While the AAP certainly endorses this type of approach centres need to be honest and disclose their success with such resuscitations. If you have zero survivors and know that there is a non standard approach at delivery of such patients and substandard equipment such as the absence of blenders to allow less than 100% O2 resuscitation do you not have a moral and ethical obligation to draw the line and say no?
The AAP offers the best approach to resuscitation from 22-25 weeks that I have seen but I don’t believe it is for every centre at the moment. Only those centres who believe that they have all the infrastructure and processes in place to achieve “perfect practice” should be routinely resuscitating infants at 22 and 23 weeks. To continue to offer these families everything and perform less than perfect practice will not lead to any improvements in their rate of success and do the families that come to their hospitals a disservice.
The first step in medicine is to pledge to do no harm. I would hope that hospitals would be honest with themselves and if they don’t have everything in place to achieve great results will spare families the experience of false hope when the only outcome will be the inevitable loss of a child.


 In April of 2015 Rysavy et al published the results of survival and morbidity data for infants born in 24 US hospitals between the ages of 22 – 26 weeks. The nearly 5000 infants included demonstrated two very important things. Firstly, survival is possible at 22 and 23 weeks and there is a chance, albeit less than 50% that these infants will survive without moderate or severe disability. Secondly, at these gestational ages 75% of hospitals included provided active resuscitation to these infants. Given that this is the largest study out there and shows that survival is possible and we can expect to see some good outcomes it would seem logical to move forward with universal resuscitation of these infants would it not?
In April of 2015 Rysavy et al published the results of survival and morbidity data for infants born in 24 US hospitals between the ages of 22 – 26 weeks. The nearly 5000 infants included demonstrated two very important things. Firstly, survival is possible at 22 and 23 weeks and there is a chance, albeit less than 50% that these infants will survive without moderate or severe disability. Secondly, at these gestational ages 75% of hospitals included provided active resuscitation to these infants. Given that this is the largest study out there and shows that survival is possible and we can expect to see some good outcomes it would seem logical to move forward with universal resuscitation of these infants would it not? This represents about a 5% increase in patient bed days per year. Five percent may not seem like a large increase at first blush but when we like many hospitals have been trying to deal with staffing issues and many days in which we are at or near capacity, this is not an insignificant challenge. It is a challenge though that we must face head on. Resources must be found, and space provided to accommodate for these children. We live in a world now where it is not solely up to us but to the family as well who must be integral to any such decision to either pursue or withdraw care. News of such infants surviving has spread to the public and I have no doubt that many families will have heard stories of such survivors. The next phase of care for these infants must address the shortcomings in care at the moment.
This represents about a 5% increase in patient bed days per year. Five percent may not seem like a large increase at first blush but when we like many hospitals have been trying to deal with staffing issues and many days in which we are at or near capacity, this is not an insignificant challenge. It is a challenge though that we must face head on. Resources must be found, and space provided to accommodate for these children. We live in a world now where it is not solely up to us but to the family as well who must be integral to any such decision to either pursue or withdraw care. News of such infants surviving has spread to the public and I have no doubt that many families will have heard stories of such survivors. The next phase of care for these infants must address the shortcomings in care at the moment.


 Failure to do so results in atelectasis.
Failure to do so results in atelectasis.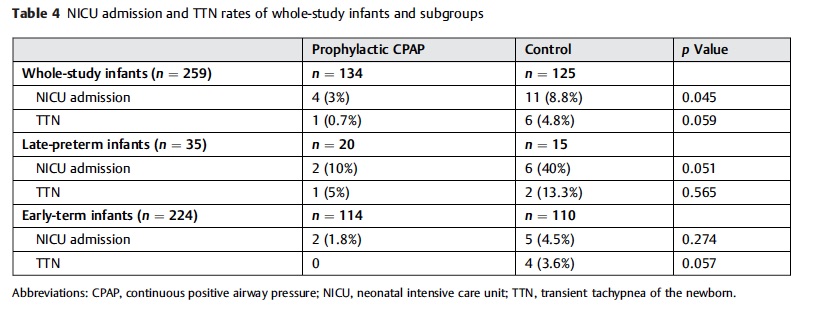 figure. The results here although just achieving significance should not be minimized. Avoiding progressive atelectasis decreases admission rates. The conclusion here is that there is little benefit in adopting a wait and see approach to those kids born by elective c-section. While it is true that you may be treating a significant number of healthy patients between 34 0/7 – 38 6/7 weeks with CPAP it is for a brief period and makes a significant difference in frequency of admission.
figure. The results here although just achieving significance should not be minimized. Avoiding progressive atelectasis decreases admission rates. The conclusion here is that there is little benefit in adopting a wait and see approach to those kids born by elective c-section. While it is true that you may be treating a significant number of healthy patients between 34 0/7 – 38 6/7 weeks with CPAP it is for a brief period and makes a significant difference in frequency of admission.
