I often catch myself saying that Neonatology being a relatively young speciality has so much more to discover. Any Pediatric resident can attest to this when they scan their journals and see so many articles exploring uncharted territory. As we continue to march forward it gave me pause to realize that we had lost someone in August who quite literally put the intensive in Neonatal Intensive Care.
Dr. Forrest Bird was an inventor and a pilot who was inspired to create a device to deliver oxygen to pilots flying at high altitude. This was needed due to the inability of the allied airforce to fly as high as the German planes. He was able to reverse engineer of sorts a solution to the lack of oxygen the airforce experienced and thereby level the playing field. This technology became the backbone behind the Bird Respirator first produced in 1950. This device is considered to be the dawn of the ventilator and was soon to put the iron lung out of business.
In 1963, following the death of John F. Kennedy’s son Patrick at 34 weeks from RDS research in the field of Neonatology blossomed bringing something positive out of tragedy. Funding for research in the area uncovered the cause of RDS as surfactant deficiency by Dr. Avery and a great number of papers followed exploring the concepts of surface tension, atelectasis and the effects of pressure on expansion of the newborn lung. While I clearly was not working in the field back then I have no doubt the clear need for a device to help these newborns with collapsable lungs inspired Dr. Bird to search for a solution. In 1970 he produced the Baby Bird Ventilator which was essentially a smaller version of the original. Up until this point, there was little that could be done for such preemies and other children in respiratory failure. By some accounts the ability to ventilate a newborn with positive pressure led to a reduction in mortality from 70% to 10% due to respiratory distress.
How Big An Impact Did It Have?
According to the World Health Organization approximately 15 Million babies are born before 37 weeks each year in the world. In the US alone about 1 in 9 babies are born at these gestational ages which translates to about 450000 babies per year. If we take a conservative estimate that 50% will have some degree of respiratory distress and need ventilation or CPAP that translates into 7.5 million babies every year helped by technology that Dr. Bird brought into this world. While true that the Baby Bird would be replaced by more advanced technology as years passed and ventilators of today bear little resemblance to the original design, every device owes a nod to the its ancestor the Baby Bird.
It has been 45 years since the Baby Bird came to market and there are few people working in the field today who would remember using this particular ventilator. Its inventor both directly and indirectly is responsible for saving the lives of millions of babies over a 45 year span. How many of us working in the field today can say that we know someone who has made such an impact in recent memory. Dr. Bird was a hero in Medicine and in particular Neonatology and for that reason in received the National Medal of Technology and Innovation from President Obama in 2009.
I hope that this piece helps to educate even a few people about this modern day hero. It also serves to remind me as we begin to lose the pioneers in our field that perhaps we aren’t such an young specialty anymore after all.
* I would like to thank Jennifer Degl for providing permission to use her photo for this post. She is the author of From Hope to Joy and does great work which can be found at: www.micropreemie.net
A publication this past week has been featured in multiple news stories across North America due to it’s impact on mortality and morbidity in the NICU. Shielding Parenteral Nutrition From Light Improves Survival Rate in Premature Infants: A Meta Analysis made the splash that it did because it’s premise is so simple yet has such an impact. In essence, protect TPN from light (including phototherapy) and you can cut mortality in the NICU in half!
A Canadian Research Story
The CBC has covered this as well with the following piece that also indicates that a survey of NICUs from 4 years ago indicated about half of hospitals did not employ such shielding. In fairness the meta-analysis has just been published which combined 4 studies and about 800 patients to yield these findings but the understanding that such practice could benefit newborns in NICU has been known for many years. What makes this story even more interesting to me is it’s Canadian origin in that Dr. Chessex performed much of the work in this field and his dedication to the area of oxidative stress in large part led to this finding.
In fact in 1999 he published the following paper Protecting solutions of parenteral nutrition from peroxidation which demonstrated that simply covering the bag of TPN was not enough to prevent oxidation from occurring. The whole set up including the bag, lines and during the preparation of TPN needed to be shielded or peroxide concentrations increased by 1.5 -2 times compared to when a clear set up was used. Furthermore phototherapy led to a further rise in the concentration of these oxidative harmful molecules. Ironically it is the necessary components of TPN including riboflavin and lipid that create the environment for light to create these oxidative products that can damage tissue.
You may ask yourself at this point why something that was known nearly 17 years ago did not lead to widespread adoption by NICUs across Canada and perhaps North America. For one, medicine is notoriously slow to change practice especially when there is an effort and cost that will need to be considered. Sourcing such materials is actually more difficult than it may seem as we learned locally two years ago when one of our hospitals began this change. Secondly, Neonatology is littered with bench research that while striking in its findings simply did not translate into a clinically relevant outcome. For example we know that phenobarbital increases the conjugation of bilirubin in the liver and therefore in theory should be a great adjunctive treatment to phototherapy for the usual newborn jaundice but that didn’t pan out in human trials. What is the story here though?
The Landmark Study Results That Made Headlines
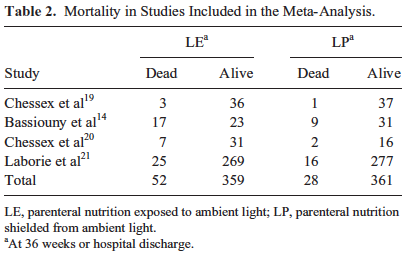
The meta-analysis mentioned in the start of this piece and causing all this attention included four studies that examined possible reductions in mortality. In 2007 Chessex studied the effect of light protection (LP) on the incidence of BPD finding a 30% reduction in those infants in a randomized study of LP vs none. This finding alone should be enough to raise some eyebrows and it did as many centres were adopting LP around this time. The second study done in Egypt in 2009 demonstrated a similar finding in reduced BPD rates. The third study was by Chessex again in 2009 and once more demonstrated reductions in oxidant stress and BPD. Curiously the largest of the studies based out of France with 587 patients in 2014 randomized to LP or none found no difference in BPD or death but the latter was very close to meeting statistical significance. In all of these studies no difference in mortality was noted however when they were combined and examined as a group the following was identified. Herein lies the power so to speak of the meta-analysis. Small studies may not demonstrate a difference that reaches significance in the desired outcome of interest but if several studies that have very similar measurements are pooled together the power to find a difference may emerge. That would seem to be the case here in that not only is there a halving of mortality that reaches statistical significance but a specific disadvantage for males was uncovered in that they had a two fold risk compared to females of dying if their TPN was uncovered.
Are These Results Relevant to Modern Practice
The results of this study are profound in terms of the impact that they could have on both BPD and mortality in our NICUs. One caveat needs to be mentioned however and that is the utlilization of oxygen in the NICU now and during the time of these studies. Since the time periods that these studies were undertaken, the use of oxygen for many units including our own has become more tightly regulated. As per NRP guidelines we resuscitate our newborns with room air and use every effort at the bedside to avoid wide swings of FiO2 when addressing an episode of desaturation. Furthermore, antenatal steroids, surfactant, liberal use of CPAP have all led to marked reductions in need for FiO2 such that the days of infants being on 30% FiO2 by nasal prongs have been replaced by room air on CPAP for the most part (at least in our units). What would these results be now if these studies were repeated? My suspicion is not as dramatic but there is no question that for at least 17 years we have known about the risk of such oxidative stress.
Is there any logic behind waiting for more evidence in a modern cohort before implementing a strategy of protecting these solutions from light? I don’t think so and hope that the rest of our community agrees and does not wait many more years to implement such precautions. How many other conditions such as ROP could be affected by simply protecting these solutions from light? Quite frankly I don’t need to know. The time has come for change.
Thank you Dr. Chessex for your dedication in bringing this translational research from the bench to the bedside.
Since that post, an incredible shift has occurred in the way that we as a team view attempts at resuscitation at 23 weeks. It took a great deal of dialogue among all health care providers and a deeper understanding of concerns of both Obstetrical and Neonatal colleagues to come to a mutual understanding that could yield a path to move forward. Through dialogue, the damage that had been done by the development of a “broken telephone” was repaired and trust emerged across disciplines which was the only way forward from the beginning.
Why not 22 weeks?
Yes, gestational age is so much more than just a number and must include estimates of fetal size, certainty of dates, parental wishes and several other factors to arrive at a decision that incorporates the wishes of the family. There are certainly significant challenges to informing families during a time of incredible stress as to the options that lay before them but we have to do our best in the time that we have.
When you are crossing that barrier of 24 weeks gestation, despite the caution above about the uncertainty surrounding gestational age dating there is a significant mental leap to move to 23 weeks. The leap to consider 22 weeks is even larger and I would suggest several fold. Is it possible that we would resuscitate such an infant? Absolutely if the dating was uncertain, the family had strong wishes and the team was on board with such a decision but for now this will not be advocated for at all in our city. I suspect similar discussions are happening all over North America and it will be fascinating to see where we land in 5, 10 and more years into the future.
What was the most important change to practice to enable progress?
Prior to 2015 we had one survivor at 23 weeks in a five year period. This year out of five actively resuscitated 3 have survived and at early assessments seem to be doing well. The overwhelming consensus was that skin care needed to be of paramount importance in this process. To that end we began a new process for cleaning the umbilical cord for line insertion with the goal to minimize skin burns on the abdomen. I am proud to report that since we change our technique there have been no skin burns found where once this was commonplace.
The process can be found in this short video here.
For now though, we are about to embark on a new journey in our city and I look forward to the continued collaboration with Obstetricians, Ethicists and all members of the Neonatal team as we explore this new frontier together.
I thought you may find it useful to see how this journey began and where we think it may go by watching this video of myself, Dr. Craig Burym (Obstetrics) and Dr. Aviva Goldberg (Ethics) presenting the approach to resuscitation at 23 weeks from the Neonatal, Obstetrical and Ethical standpoints. The video is about 50 minutes in length but truly addresses issues from multiple vantage points so if you missed it or are interested in how these issues were dealt with please have a look.
(If you are watching this on an Apple computer please use Safari to view)
Nick is a tremendous advocate for premature infants and their families everywhere and as President and Co-Founder of Graham’s Foundation certainly puts himself front and centre. For more information on the incredible work he and his team are doing please see their website at and if you are in the New York area please consider attending their charity benefit to help raise some funds to continue the work that they do.
As it pertains to his question though it did get me thinking. How does a National body like the AAP determine best practice suggestions for a country with 50 states in which roughly 320 million people reside? Using 2013 USA census data ,showing 23.1% of it’s citizens are under 18 this equates to nearly 74 million children. This is a daunting task no doubt and due to regional variation in terms of expertise and available resources not all policies or guidelines are possible to implement equally or at all.
The article that is being addressed in his question of the day is from Med City News which addresses the latest statement from the AAP on managing an anticipated birth before 25 weeks. For the actual statement that the article refers to please see this link which will direct you to the actual paper.
When the Canadian Pediatric Society (CPS) reaffirmed their statement in January 2015 it drew a fair bit of criticism from Canadian Neonatologists and others from abroad due to it’s draconian approach to infants at 22 and 23 weeks gestation. In the CPS statement the following was written in the recommendations section with respect to these two gestational ages which also encompassed 24 weeks as well.
“At 22 weeks’ GA since survival is uncommon, a non-interventional approach is recommended with focus on comfort care”
“At 23 and 24 weeks’ GA active treatment is appropriate for some infants”
What drew the ire of these health care providers was the apparent limitation of resuscitation based on gestational age. It did not seem that consideration was being given to potential inaccuracies with gestational age dating which at best in the first trimester are +/- a few days and in the second trimester may be off up to 1-2 weeks. Furthermore no mention was made of accounting for other factors such as the findings on an ultrasound which if very discrepant might suggest an older fetus or perhaps equally important the wishes of the parents. What were their past experiences, religious beliefs or lengths to which they had tried for this pregnancy. The 16 year old single mother who conceived via rape might be expected to have a vastly different perspective than the mother at 43 who has tried 5 rounds of IVF and has finally conceived her first baby. Many of these points were highlighted in a response by a large group of care providers in a paper entitled “CPS position statement for prenatal counselling before a premature birth: Simple rules for complicated decisions.”
Now we have a new statement from the American Academy of Pediatrics which I have to complement as it addresses a number of concerns that the above group had with the Canadian version.
1. Fetal gestational age, as currently estimated, is an imprecise predictor of neonatal survival, but 22 weeks of gestation is generally accepted as the lower threshold of viability.
2. Although most infants delivered between 22 and 24 weeks’ gestation will die in the neonatal period or have significant long-term neurodevelopmental morbidity, outcomes in individual cases are difficult to predict.
3. Outcomes of infants delivered at 22 to 24 weeks of gestation vary significantly from center to center.
4. Because of the uncertain outcomes for infants born at 22 to 24 weeks’ gestation, it is reasonable that decision-making regarding the delivery room management be individualized and family centered, taking into account known fetal and maternal conditions and risk factors as well as parental beliefs regarding the best interest of the child.
The first four points address the issues of uncertainty in dates, variable outcomes and the importance of taking a family centred approach. On the surface this seems like the perfect statement but I have highlighted the third point as it really gets to what Nick Hall is referring to (or at least my interpretation). We know that there is a great variability in outcomes from 22-26 weeks across the US based on the recent study by Rysavy et al. In this study which involved 24 hospitals with tertiary care centres, the median survival across all hospitals at 22 weeks (who actively resuscitated infants) ranged from 0 – 14.6% and at 23 weeks 23.8 – 37.1%. Imagine you are a parent at a centre that has a zero percent survival rate at 22 weeks. Should the hospital inform you of that and if after hearing that you still want “everything done” should the Neonatal team resuscitate your infant? There is no doubt that the parental wishes as outlined in point 4 are important but I would counter that there is also little point in putting a family through a futile exercise.
Vince Lombardi the former head coach of the Green Bay Packers produced the following quote that has been used many times since his heyday in the 1960s. “Practice does not make perfect. Only perfect practice makes perfect”
This could not be more applicable to the situation in many centres thoughout the US. Resuscitating 22 and 23 week infants can be done and in a manner of speaking is a form of practice. Should centres though who have not “perfected” their approach by having rigorous audits of their practice, a “golden hour” approach and lastly the best equipment for resuscitation continue to offer families who wish to “do everything” just that? I would say no. While the AAP certainly endorses this type of approach centres need to be honest and disclose their success with such resuscitations. If you have zero survivors and know that there is a non standard approach at delivery of such patients and substandard equipment such as the absence of blenders to allow less than 100% O2 resuscitation do you not have a moral and ethical obligation to draw the line and say no?
The AAP offers the best approach to resuscitation from 22-25 weeks that I have seen but I don’t believe it is for every centre at the moment. Only those centres who believe that they have all the infrastructure and processes in place to achieve “perfect practice” should be routinely resuscitating infants at 22 and 23 weeks. To continue to offer these families everything and perform less than perfect practice will not lead to any improvements in their rate of success and do the families that come to their hospitals a disservice.
The first step in medicine is to pledge to do no harm. I would hope that hospitals would be honest with themselves and if they don’t have everything in place to achieve great results will spare families the experience of false hope when the only outcome will be the inevitable loss of a child.
During a recent trip to Italy I couldn’t help but notice how common smoking continues to be in this country. From speaking with several people there I also understand it is not uncommon in many countries throughout Europe. Thankfully many countries are introducing smoke free legislation and as a Neonatologist I couldn’t be happier. I doubt there is anyone out there who would suggest that smoking is not without risk in pregnancy. Those who persist in this habit may argue that the risks are overstated but it would be tough to argue that there are no increased risks at all.
While taking a break from enjoying the sites that Italy has to offer I came across an article published in Nature this past week entitled “Impact of smoke-free legislation on perinatal and infant mortality: a national quasi-experimental study” addressing the impact of smoking on stillbirth and newborn death rates in England. Examining the period from 1995 – 2011 which included the introduction of smoke-free legislation in 2007 the authors demonstrated immediate and dramatic benefits to pregnancies in England The study was massive with 52,163 stillbirths matched to 10,238,950 live-births.
Impact of Smoke Free Legislation
Smoke-free legislation was associated with an immediate 7.8% (95%CI 3.5–11.8; p < 0.001) reduction in stillbirth, a 3.9% (95%CI 2.6–5.1; p < 0.001) reduction in low birth weight, and a 7.6% (95%CI 3.4–11.7; p = 0.001) reduction in neonatal mortality.
As if those numbers isn’t impressive enough, in the four years following the legislation it is estimated that this translated into 991 less stillbirths, 5470 cases of low birth weight (many of whom would need admission) and 430 less neonatal deaths!
Surely this would translate into a dramatic reduction in women who smoke but sadly at least in many parts of the world it does not.
While many women quit in anticipation of an upcoming pregnancy or once they find out they are pregnant, many more do not. In several studies the percentage of women who quit smoking after the first pregnancy ranges from 25-31%.
Complications such as increased rates of stillbirths, fetal growth restriction and hypertension I thought would lead a woman to clearly choose to stop before the next pregnancy but as mentioned this is not the case in the majority of pregnancies. In no way do I believe that such women are immoral or insensitive to the risks to their babies but rather this underscores the severity of the addiction that such women face. I continue to be amazed at what women will subject themselves to in order to protect the life growing inside them but when it comes to keeping a stick of burning tobacco out of their mouths many are incapable.
How Successful Are Women At Quitting From One Pregnancy to The Next
DT Tran and colleagues examined an Australian cohort of women in a paper entitled “Change in smoking status during two consecutive pregnancies: a population-based cohort study”. The authors had the benefit of having access to a very well-organized database in Australia and were able to examine 183385 women who had subsequent pregnancies and determine those who were smokers and then quit for the second and those who were not and took up the habit in the second pregnancy. The data they use has been shown in previous work to be highly reliable in terms of accuracy of maternal smoking status during pregnancy.
They were curious to see how Australia’s campaign against tobacco use in pregnancy had been working so wished to compare smoking cessation rates with other previously reported populations. ]Overall 33.5% of women who smoked in a first pregnancy quit before the next one and of those who never smoked in the first pregnancy 3.6% smoked in the second. These results are somewhat better than those previously reported but certainly do not shoot the lights out in terms of effectiveness.
It was their additional finding however that I found intriguing and wished to share as I believe it is quite interesting and allows for some speculation. Mothers who were >24 years old, married, born in a non-english speaking country or lived in a higher social demographic were more likely to quit. Additionally, mothers who had an inter-pregnancy interval of 3 years or longer were more likely to quit. There may not be much surprise there as the older mother who has obtained a little more wisdom and is less inclined to be swayed by peer pressure may also be more successful in quitting. Furthermore, mothers who are pregnant less frequently may have more time to quit and moreover come from a higher demographic population depending on circumstance.
Motivating Factors to Quit
What was unusual though in this population was the finding that mothers who had experienced gestational hypertension, had a stillbirth or an LGA infant were more likely to quit while those who had an SGA infant or had an infant admitted to NICU were less likely to quit. For women who took up the habit in the second pregnancy, late seeking of prenatal care, gestational diabetes, preterm birth, C/S, SGA infants and a previous infant admitted to NICU were all risk factors for starting to smoke. All of these factors showed statistical significance.
From this very large population cohort it would seem that having lost an infant as a stillbirth is a very compelling reason to quit but having had a small baby or one admitted to the NICU is not. There has been much talk about smoking and the risks of stillbirth as mentioned in the article at the start of the piece but I suspect the risks of small babies or those needing NICU admission has not garnered the same attention.
There is not much that we as Neonatal care providers can do prior to admission to the NICU but perhaps for those who are admitted and are born to mothers that smoke there is an opportunity here for advocacy. It may well be that we as practitioners have been unaware of the impact of smoking on our resources. NICUs around the world are running out of room and in need of expansion due to continuing demand. I think the time has come to identify these women in hospital and talk to them about smoking as part of discharge planning. We do this of course for our kids with BPD as we worry about their lung function in a smoke-filled environment but can we as providers do a little more to educate those who seemingly are not as high risk (think the 1900g SGA infant) and help get them on track with a smoking cessation program? As you can tell I think the answer is yes and it is a little something each of us should do as together it may have a large impact on a global scale.
As I write this post the stock markets in around the world are in a free fall. The DOW Jones is down nearly 1000 points and with it I can only imagine the mood of those in business around the globe. I find myself though rather calm this morning as I write this, not because I am not exposed to the stock market, but due to the safety that exists in the health care sector.
I recall vividly on the opening day of medical school hearing the Dean of Medicine say the following.
“If any of you applied to Medicine to earn a lot of money I would like you to take a look at the exit doors and consider walking out and going to the school of Business. This is where true wealth is created”
As you can tell I didn’t run for the door but over the next few years I did watch as friends who went through the business world achieved remarkable things in terms of status that I could only dream of. Homes, cars, toys, you name it, they came early to those who avoided the lengthy and poorly paid course of medicine. Eventually though that all ended when I finally finished and entered the working world but there is no question that the Dean was right. You see in Medicine, especially Neonatology we don’t have what you would call scalable earnings. I can’t create more supply of babies and even if I could it would not be without doing a lot of extra work. Also, there are only 24 hours in a day so really there is a limit to how many patients I can see and there is a linear relationship with workload. Contrast that with someone in business who is selling a gadget. It doesn’t take twice the work to ship twice the number of gadgets therefore it is scalable and very profitable. The downside though is that when the demand for the gadgets drops off in times of financial crisis such as “Black Monday” your profits and income can drop as quickly as they have risen.
As I sit and write this today I am grateful that I work in this non-scalable industry of health care and more specifically Neonatology. As long as I do a good job and continue to work I think there is little risk of a contracting workforce. There is a risk that a drop in birth rate or marked reduction in admissions due to a reduction in premature birth could lessen the need for my profession but I don’t see that happening any time soon. All indications in the media, through health care benchmarking and by my own eyes tell me that my job is fairly secure.
It is human nature though to covet those things that we don’t have or can’t reach. I won’t have a private jet, mansion on the ocean or the ability to drink the finest wines as my everyday stock but I do have something far better. I take care of newborns and their families. I love what I do and barring any of the above changes in demand for my services I will be able to do this and earn a decent living from it until I am long in the tooth. Whether you are a Neonatal nurse, dietician, RRT or any one of a number of the critical pieces that help run the NICU on a daily basis be grateful for what you have. No one can take it away from you whether the markets are up, down or sideways.
Lastly while those in business today are staring at this.
Be very glad that every day we get to stare at this…
Any concerns you have had with this turmoil will feel a lot better when you just turn your head from the screen and look at the baby in front of you. We have a job to do and if we stick to it we will accomplish great things for babies and families while providing safely for our own families.


 In 1970 he produced the Baby Bird Ventilator which was essentially a smaller version of the original. Up until this point, there was little that could be done for such preemies and other children in respiratory failure. By some accounts the ability to ventilate a newborn with positive pressure led to a reduction in mortality from 70% to 10% due to respiratory distress.
In 1970 he produced the Baby Bird Ventilator which was essentially a smaller version of the original. Up until this point, there was little that could be done for such preemies and other children in respiratory failure. By some accounts the ability to ventilate a newborn with positive pressure led to a reduction in mortality from 70% to 10% due to respiratory distress.
 Herein lies the power so to speak of the meta-analysis. Small studies may not demonstrate a difference that reaches significance in the desired outcome of interest but if several studies that have very similar measurements are pooled together the power to find a difference may emerge. That would seem to be the case here in that not only is there a halving of mortality that reaches statistical significance but a specific disadvantage for males was uncovered in that they had a two fold risk compared to females of dying if their TPN was uncovered.
Herein lies the power so to speak of the meta-analysis. Small studies may not demonstrate a difference that reaches significance in the desired outcome of interest but if several studies that have very similar measurements are pooled together the power to find a difference may emerge. That would seem to be the case here in that not only is there a halving of mortality that reaches statistical significance but a specific disadvantage for males was uncovered in that they had a two fold risk compared to females of dying if their TPN was uncovered.






