It isn’t often that something comes along that causes me to raise not one but two eyebrows but I suppose the idea of adding insulin to preemies feeds is just such a thing. Apparently this research isn’t that new as there has been some previous animal research and human testing of breastmilk that revealed insulin is present in milk at concentrations of 46 microunit/mL. Testing of amniotic fluid has found even higher levels at 2500 microunits/mL! All of this insulin can’t be there by accident. If you believe in evolution as I do it can’t be by chance that all that insulin doesn’t have a role to play. By extension, since babies swallow amniotic fluid and therefore bath the developing intestine in insulin containing fluid there must be a benefit right?
Let’s do a study looking at benefits of oral insulin added to formula!
Researchers in Israel thought the same thing as they postulated that since insulin is a growth factor in the intestine that adding an oral formulation to formula may confer benefits. We know that breastmilk is better tolerated by preemies and might it be that the growth promoting effects of insulin in breastmilk is a contributing factor? There had already been a proof of concept Phase 1 study to test the use of oral insulin at 400 microunit/mL so on this go around the authors sought to perform a larger Phase 2 study looking at the primary outcome of time to full feeds. The paper is entitled Efficacy and Safety of Enteral Recombinant Human Insulin for Reduction of Time-to-Full Enteral Feeding inPreterm Infants: A Randomized, Double-blind, Placebo-Controlled Trial.
Infants included in this study were from 26-33 weeks GA with a birth weight greater than or equal to 750g and postnatal age < 7 days. Since breastmilk has insulin in it already all infants were fed formula. The insulin was NTRA as a dry powder with the dose of 400 microunit/mL chosen based on the amount known to be in amniotic fluid. The study required 76 patients but was stopped after 33 patients when a planned interim analysis found a benefit already to the intervention without any safety concerns identified.
The Results
The primary outcome was the time it took to reach full feedings defined as 150 mL/kg/d of enteral formula intake.
As you can see there was about a 1.6 day advantage favouring the group receiving insulin. This represents a 20% reduction in time to full feedings
In terms of secondary outcomes the results were also impressive even more so when one considers the small sample size. While we don’t routinely measure gastric residuals in our centre the authors did these measurements as a proxy for feeding tolerance. They defined low residuals as a goal of < 2 mL/kg in 24 hours. In the insulin group this goal was reached in 1.67 days vs 5.09 days in the placebo group. While this result had a p Value of 0.056 so therefore just missed being significant it is an interesting trend for sure. Again owing to small size while a difference in time to wean off TPN was 2.4 days shorter in the insulin group it was not significantly different. No difference it time to discharge was found but again the difference favoured the insulin group with a mean reduction of about 9 days for singletons.
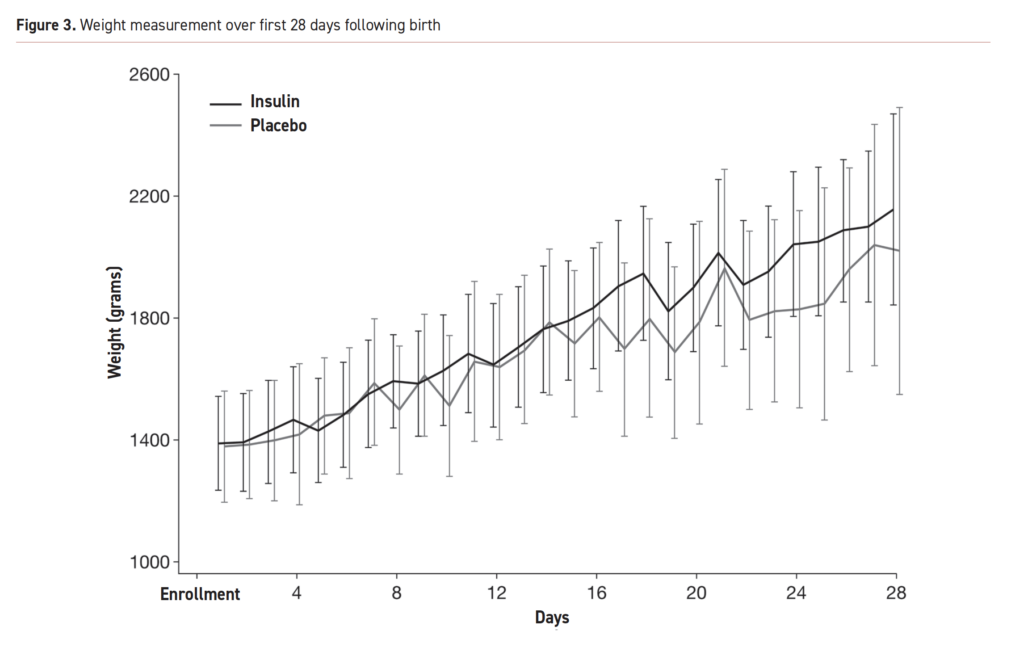
Below are the growth curves for the first 28 days reflecting a mean weight increase of 768.9g in the insulin group and 643.6g in the placebo arm.
So What’s Next?
I would like to start of by saying I hope one day you say you saw it here first! I think this research is very promising and no doubt a phase 3 trial with larger numbers is on the way. This isn’t quite ready for prime time as the saying goes based on small numbers but it is reassuring. Keep in mind this isn’t for everyone. We want as much as possible to provide breastmilk to our infants as it is more than just growth that we think about and time to full feeds. The question though for the future is whether for mothers who can’t produce enough or don’t want to breastfeed whether a little insulin sprinkled into their infant’s feeding will be just what the doctor ordered. My bet is that in the future you will see this indeed come into practice but we will need to certainly wait for bigger trials to confirm the trends that we are seeing here!@
This could turn into a book one day I suppose but I have become interested in chalenging some of my long held beliefs these days. Recently I had the honour of presenting a webinar on “Dogmas of Neonatology” for the Indian Academy of Pediatrics which examined a few practices that I have called into question (which you can watch in link). Today I turn my attention to a practice that I have been following for at least twenty years. I have to also admit it is something I have never really questioned until now! In our institution and I suspect many others, infants born under 1250g have been fed every two hours while those above every three. The rationale for this has been that a two hour volume is smaller and causes less gastric distention. This in theory would benefit these small infants by helping to not compromise ventilation or lead to reflux. Overwhelming the intestine with large distending boluses would also in theory lead to less necrotizing enterocolitis. All of this of course has been theoretical and I can thank those who preceded me in Neonatology for coming up with these rules!
Study Challenges This Old Belief
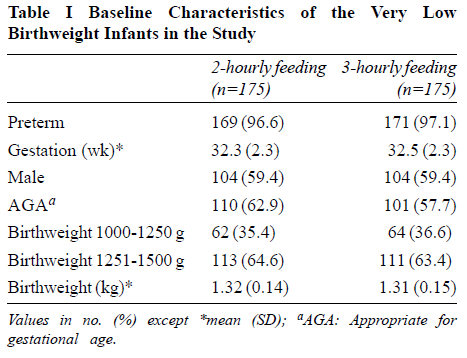
Yadav A et al published Two-hourly versus Three-hourly Feeding in Very Low Birthweight Neonates: A Randomized Controlled Trial out of India (well timed given my recent talk!). The authors randomized 175 babies born between 1000-1500g to either be fed q2h vs q3h once they began protocol feeding. The primary outcome was time to full feedings. Curiously, the paper indicates they decided to do a preplanned subgroup analysis of the 1000-1250 and 1251 -1500g groups but in the discussion it sounds like this is going to be done as a separate paper so we don’t have that data here.
The study controlled conditions for determining feeding intolerance fairly well. As per the authors:
“Full enteral feed was defined as 150 mL/Kg/day of enteral feeds, hypoglycaemia was defined as blood glucose concentration <45mg/dL [15]. Feed intolerance was defined as abdominal distension (abdominal girth ≥2 cm), with blood or bile stained aspirates or vomiting or pre-feed gastric residual volume more than 50% of feed volume; the latter checked only once feeds reached 5 mL/kg volume [16]. NEC was defined as per the modified Bells staging.”
We don’t use gastric residuals in our unit to guide cessation of feedings anymore but the groups both had residuals treated the same way so that is different but not somethign that I think would invalidate the study. The patients in the study had the baseline characteristics shown below and were comparable.
Results
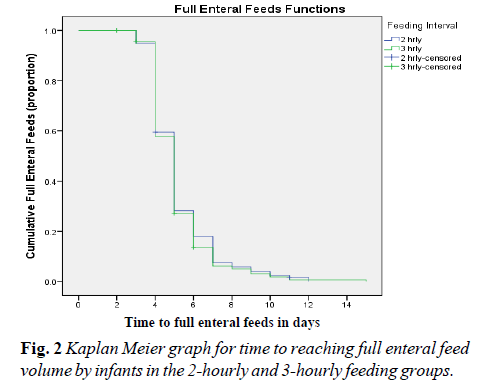
It will be little surprise to you that the results indicate no difference in time to full feedings as shown in Figure 2 from the paper.
The curves for feeding advancement are essentially superimposed. Feeding every two vs three hours made no difference whatsoever. Looking at secondary outcomes there were no differences as well in rates of NEC or hypoglycemia. Importantly when examining rates of feeding intolerance 7.4% of babies in the 2 hour and 6.9% in the 3 hour groups had this issue with no difference in risk observed.
Taking the results as they are from this study there doens’t seem to be much basis for drawing the line at 1250g although it would still be nice to see the preplanned subgroup analysis to see if there were any concerns in the 1000-1250 group.
Supporting this study though is a large systematic review by Dr. A. Razak (whom I have collaborated with before). In his systematic review Two-hourly versus three-hourly feeding in very low-birth-weight infants: A systematic review and metaanalysis. he concluded there was no difference in time to full feeds but did note a positive benefit of q3h feeding in the 962 pooled infants with infants fed 3-hourly regainin birth weight earlier than infants fed 2-hourly (3 RCTs; 350 participants; mean difference [95% confidence interval] -1.12 [-2.16 to -0.08]; I2 = 0%; p = 0.04). This new study is a large one and will certainly strengthen the evidence from these smaller pooled studies.
Final Thoughts
The practice of switching to q2h feedings under 1250g is certainly being challenged. The question will be whether the mental barriers to changing this practice can be broken. There are many people that will read this and think “if it’s not broken don’t fix it” or resist change due to change itself. The evidence that is out there though I would submit should cause us all to think about this aspect of our practice. I will!
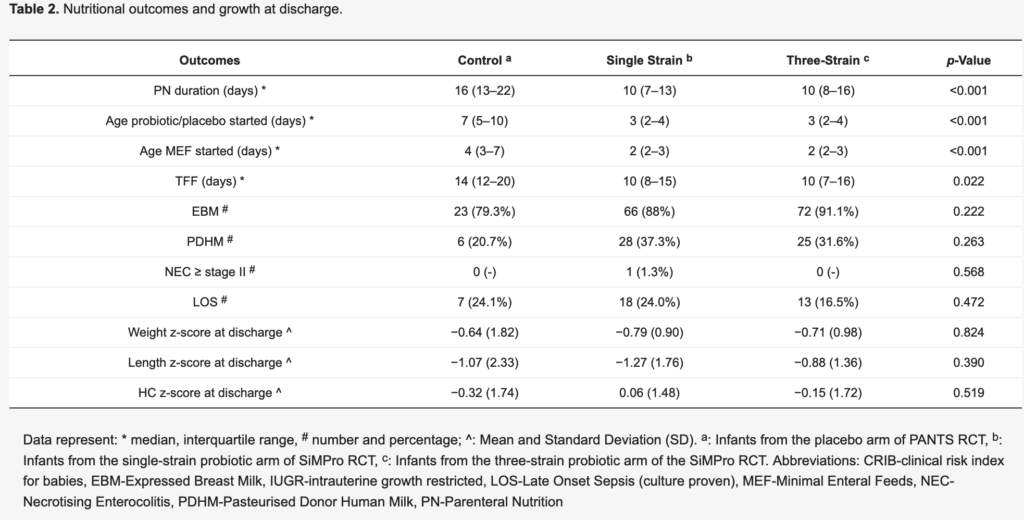
Any regular reader of this blog will know that human milk and the benefits derived from its consumption is a frequent topic covered. As the evidence continues to mount it is becoming fairly clear that the greater the consumption of mother’s own milk the better the outcomes appear to be with respect to risks of late onset sepsis or BPD as examples. Moving to an exclusive human milk diet has been advocated by some as being the next step in improving outcomes further. While evidence continues to come suggesting that replacement of fortification with a human based instead of a bovine based fortifier may improve outcomes, the largest studies have been retrospective in nature and therefore prone to the usual error that such papers may have.
What is evident though as the science pursues this topic further is that the risk of necrotizing enterocolitis or NEC is not zero even with a human milk diet. Why is that? It might be that some risks for NEC such as intestinal ischemia or extreme prematurity simply are too much to overcome the protective effect of breastmilk. Perhaps though it could be related to something intrinsic in the breastmilk that differs from one mother to another with some producing more protective milk than others.
Secretors vs Non-secretors
When it comes to the constituents of breastmilk, human milk oligosaccharides or HMOs are known to be secreted into breastmilk differently depending on whether a mother has a secretor gene or not. this has been demonstrated recently in HMOs affecting the microbiome in infants Association of Maternal Secretor Status and Human Milk Oligosaccharides With Milk Microbiota: An Observational Pilot Study. HMOs are capable of a few things such as stimulating growth of beneficial microbes and acting as “receptor decoys” for pathogenic bacteria. Previous rat models have also demonstrated their potential to reduce NEC in rat models. Essentially, mothers who have the secretor gene produce more diverse types of HMOs than mothers who are secretor negative.
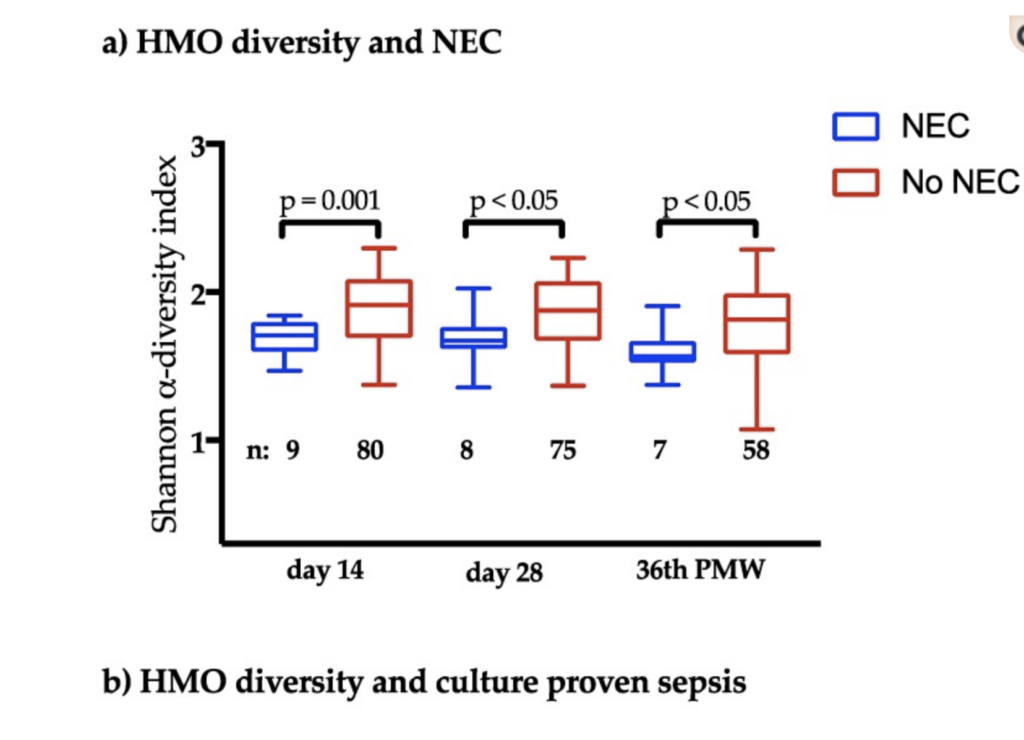
The Type of HMO May Be the Key To Reducing NEC Wejryd E et al in 2018 published Low Diversity of Human Milk Oligosaccharides is Associated with Necrotising Enterocolitis in Extremely Low Birth Weight Infants This paper was an offshoot of the PROPEL study on the use of prophylactic probiotcs to reduce severe morbidities. Babies were all born between 23 + 0 to 27 +6 weeks and all infants received exclusive breastmilk. All fortification was with a bovine product. Breastmilk samples were obtained from 91 mothers of 106 infants at 2 weeks, 28 days after birth and finally at 36 weeks PMA and the HMO content analyzed.
What came out of the study were a couple very interesting findings. The first is that when analyzing the HMOs present in breastmilk at 2 weeks and comparing those who developed NEC to those who did not there was one significant difference. Lacto-N-difucohexaose I (LNDH I)had a median level of 0 (IQR 0-213) from the milk of those mothers who had infants affected by NEC. There were no differences observed for any other HMOs.
Also of interest was the greater diversity of HMOs present in the breastmilk samples of mothers whose infants did not develop NEC. This was present at all time points.
How Could This Be Useful?
If a broader array of HMOs is associated with less risk of NEC and the presence of LNDH I carries the same association it opens the door to the next phase of this research. Could provision of LNDH I in particular but moreover a wide array of HMOs to mother’s milk reduce the occurrence of NEC? This will need to be tested of course in well designed randomized trials but this type of fortification could be the next step in what we add to human milk to enhance infant outcomes. Given that it may be difficult to determine in short order whether women have these HMOs already a broad based fortification strategy assuming insufficient amounts of HMOs would be best. A quick search on clinicaltrials.gov shows that there are 101 trials in children looking at HMOs at the moment so more information on this topic is certainly on the way. Could HMOs be the magic bullet to help reduce NEC? Just maybe!
In recent years we have moved away from measuring and reporting gastric residuals. Checking volumes and making decisions about whether to continue feeding or not just hasn’t been shown to make any difference to care. If anything it prolongs time to full feeds without any demonstrable benefits in reduction of NEC. This was shown in the last few years by Riskin et al in their paper The Impact of Routine Evaluation of Gastric Residual Volumes on the Time to Achieve Full Enteral Feeding in Preterm Infants. Nonetheless, I doubt there is a unit in the world that has not had the following situation happen. It is 2 AM and the fellow on call is notified that they need to come and see a patient. On arrival the bedside nurse shows them a syringe that contains dark green murky fluid. The fellow is told that NG tube placement was just being checked and this is what was aspirated. The infant is fine in terms of exam but the question is asked “What should I do with this fluid”. The decision is made that the fluid looks “gross” and they discard it and then decide to resume feedings with a fresh batch of milk. Both parties feel good about discarding what looked totally unappealing for anyone to ingest and the night goes on. If this sounds familiar it should as I suspect this happens frequently.
Logical Fallacy
A colleague of mine introduced me to this concept and I think it may apply here. Purdue University’s writing lab defines a Logical Fallacy in this way “Fallacies are common errors in reasoning that will undermine the logic of your argument. Fallacies can be either illegitimate arguments or irrelevant points, and are often identified because they lack evidence that supports their claim.”
I think we may have one here that has pervaded Neonatology across the globe. Imbedded in the fallacy is the notion that because the dark green aspirates look gross and we often see such coloured aspirates in patients with necrotizing enterocolitis or other bowel disease, all green aspirates must be bad for you. The second fallacy is that the darker the aspirate the more seriously you should consider discarding it. This may surprise you but on their own there isn’t much of anything that has been shown to be wrong with them. Looking for evidence to demonstrate increased rates of NEC or other abdominal issues in an otherwise well patient finds pretty much nothing to support discarding.
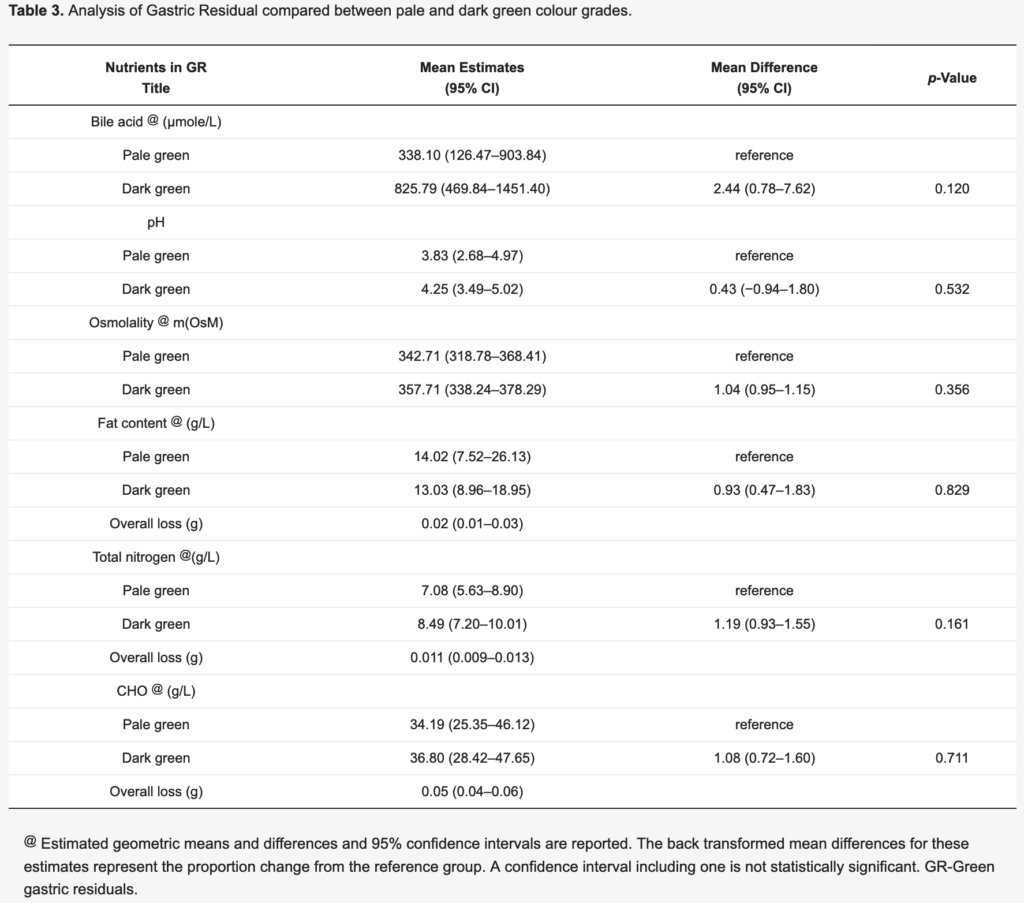
The main reason for the share of this paper is what is in Table 3.
Although not significantly different the mean estimates for concentration of bile acids in the pale and dark green aspirates came close to being different. Other nutritional content such as fat, protein and carbohydrate were no different. As the bile became darker though the bile acids tended to increase. It is this point that is worthy of discussion.
A Breakdown of the Aspirate
I’m with you. When you look at that murky dark green fluid in the syringe it just seems wrong to put that back into a belly. Would you want to eat that? Absolutely not but when you break it down into what is in there, suddenly it doesn’t seem so bad. We assume that we would not want to refeed such putrid looking material and that is where the logical fallacy exists. What evidence do we have that refeeding that fluid is bad? As I said above not much at all. Looking at the fact that there is actual nutritional calories in that fluid and bile acids as well you come to realize that throwing it away may truly not be in the best interest of the baby. Calories may wind up in the garbage and along with them, bile acids.
Bile acids are quite important in digestion as they help us digest fat and moreover as they enter the ileum they are reabsorbed in large quantities which go to further help digestion. In addition bile acid concentrations are what helps draw fluid into bile and promotes bile flow. By throwing these bile acids out we could see lower bile volumes and possible malabsorption from insufficient emulsification of fat.
The other unmeasured factors in this fluid are the local hormones produced in the bowel such as motilin which helps with small bowel contractility. Loss of this hormone might lead to impairment of peristalsis which can lead to other problems such as bacterial overgrowth and malabsorption.
Now all of this is speculative I will admit and to throw out one dark green aspirate is not going to lead to much harm I would think. What if this was systematic though over 24 or 48 hours that such aspirates were being found and discarded. Might be something there, What I do think the finding of such aspirates should trigger however is a thorough examination of the patient as dark green aspirates can be found in serious conditions such as NEC or bowel perforation. In the presence of a normal examination with or without laboratory investigations what I take from this study is that we should question are tendency to find and discard. Maybe the time has come to replace such fear with a practice of closing our eyes and putting that dark green aspirate right back where it came from.
I presented this topic as a fellow many years ago after a paper came on the scene suggesting better outcomes with a faster approach. The paper Randomized trial of “slow” versus “fast” feed advancements on the incidence of necrotizing enterocolitis in very low birth weight infants. was plagued by the same issue as others created around those years which was a small number of patients at the lowest gestational ages. Any differences in sub analyses were difficult to really believe as the outcomes could have easily been explained by chance. Having said that, many centres began advancing feeds a little faster than the typical 20 ml/kg/d in favour of 30 ml/kg/d. It would take some time to coordinate a trial large enough to really answer questions about relevant issues such as time to developmental outcomes, time to full feedings and rates of NEC and the time appears to be now.
The SIFT trial
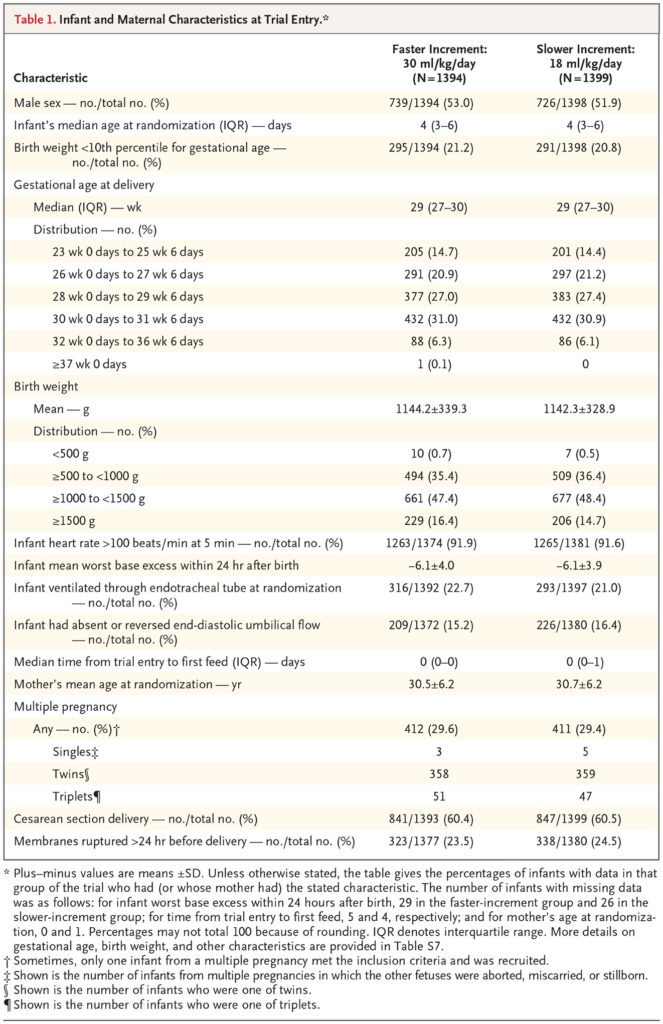
This trial (Controlled Trial of Two Incremental Milk-Feeding Rates in Preterm Infants) was the result of a great deal of coordination between 55 different centres. For inclusion, infants had to be <1500g and <32 weeks gestational age at birth. Once the decision was made to advance feeds, babies were randomized to receive increases of 18 mL/kg/d vs 30 ml/kg/d. The primary outcome was survival without mod-erate or severe neurodevelopmental disability at 24 months CGA. What is striking about the study is its size. The number of babies in the fast arm was 1394 while 1399 in the slower group. In terms of having sufficient numbers of infants who were at the earliest gestational ages they were able to accomplish this as shown in this table.
Importantly when looking at the primary outcome 87.4% of infants in the faster group vs 88.7% in the slower group were followed up for assessment. It is also worth mentioning that this is even more impressive in terms of retention when one considers that about 6% in both arms died before assessment.
What were the findings then?
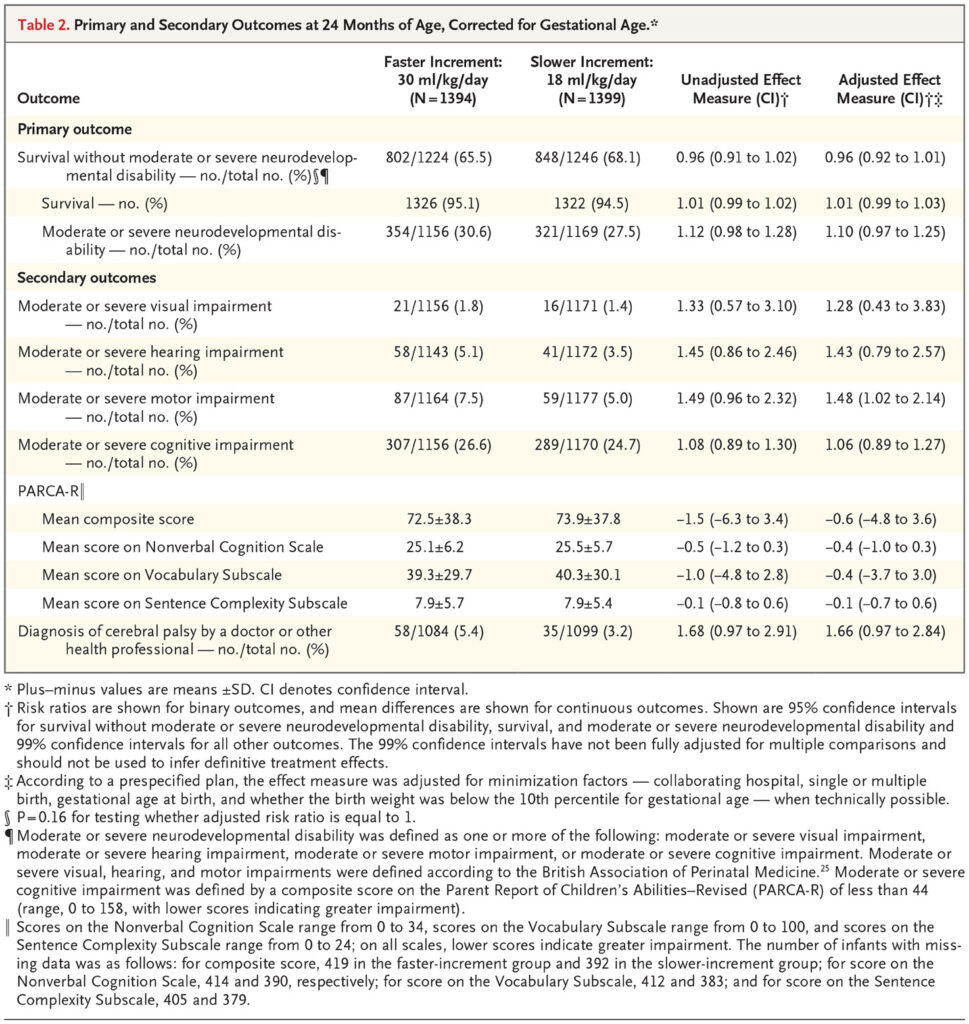
There was no difference in the primary outcome or for that matter each of its’ competing parts.
The authors in a secondary analysis did show a very marginal significant finding favouring slow feeds with respect to motor outcome. I concur with the authors though that given the small effect size and the “fishing” for results this likely is simply a chance finding. I can’t think of any reason why that would be the case either from a biological standpoint.
Not surprisingly another significant finding was shorter durations to reach full feeds (10 vs 7 days) and days on TPN at 11 vs 9 in the slow vs fast groups. In spite of having less need for central venous access, the authors were unable to show a reductoin in late onset sepsis or NEC.
Does it change your management?
I suppose that depends on what your management currently is. If you are like our centre and already advancing feedings by 30 ml/kg/d then I suspect not much. If you are in a slow centre one can take away from this study that at the very least you can lessen your patient’s need for central venous access and TPN. Based on this study and my suspicion that there will be no bigger trial forthcoming, whatever you decide to do this is about the best data that you will be getting.
The medical term for this is placentophagy and it is a real thing. If you follow the lay press you may have seen that originally this was promoted by Kourtney Kardashian who did this herself and then by Kim who planned on doing the same after delivery. See Did Kourtney Kardashian Eat Her Placenta?
This is not completely without basis as many readers will be thinking already that they have heard about the health benefits of doing the same. Reports of improved mood and reductions in the baby blues following ingestion of placenta as well as improvements in breast milk production have led to this growing practice. The evidence for this up until recently though was quite old and fraught with poorly design of such studies. The bigger driver however has been word of mouth as many women having heard about the promises of better mood at the very least have thought “why not? Can’t hurt.”
What I will do in this post is run through a little background and a few recent studies that have shed some light on how likely this is to actually work.
Where did the idea come from?
Animals eat their placentas after delivery. It turns out that unprocessed placenta is quite high in the hormone prolactin which is instrumental for breastfeeding. Given the large amount of this hormone as well as the number of other hormones present in such tissue it was thought that the same benefits would be found in humans. Eating unprocessed human tissue whether it is put in a capsule or not is unwise as unwanted bacteria can be consumed. In fact, a case of GBS sepsis has been linked to such a practice in which the source of the GBS was thought to be due to contaminated unprocessed maternal placenta that had been ingested. Buser GL, Mat´o S, Zhang AY, Metcalf BJ, Beall B, Thomas AR. Notes from the field: Late-onset infant group B streptococcus infection associated
with maternal consumption of capsules containing dehydrated placenta.
What happens when you process placenta by steaming and drying?
This would be the most common way of getting it into capsules. This process which renders it safe to consume may have significant effects on reducing hormonal levels.This was found in a recent study that measured oxytocin and human placental lactogen (both involved positively in lactation) and found reductions in both of 99.5% and 89.2%, respectively compared versus raw placenta. I would assume that other hormones would be similarly affected so how much prolactin might actually wind up in these capsules after all?
Clinical Randomized Double Blind Controlled Trial
Twenty seven women from Las Vegas were recruited into a pilot trial (12 beef placebo vs 15 steamed and dried placenta) with the authors examining three different outcomes across three studies. The first study Effects of placentophagy on maternal salivary hormones: A pilot trial, part 1 looked at a large number of salivary hormones at four time points. Plasma samples were taken as well to determine the volume of distribution of the same. First samples were at week 36 of gestation then within 4 days (96 h) of birth followed by days 5–7 (120–168 h) postpartum and finally Days 21–27 (504–648 h) postpartum. All consumption of capsules was done in the home as was collection of samples. As per the authors in terms of consumption it was as follows “two 550 mg capsules three times daily for the first 4 days; two 550 mg capsules twice daily on days 5 through 12, and then to decrease the dose to two 550 mg capsules once daily for the remainder of the study (days 13 through approximately day 20 of supplementation).
Outcomes
No difference was found between salivary concentrations of hormones at any time point other than that with time they declined following birth. Curiously the volume of distribution of the hormones in serum was slightly higher in the placenta capsule groups but not enough to influence the salivary concentrations. It was felt moreover that the amount of incremental hormone level found in the serum was unlikely to lead to any clinical response.
The second study was on mood Placentophagy’s effects on mood, bonding, and fatigue: A pilot trial, part 2. Overall there were no differences for the groups but they did find “some evidence of a decrease in depressive symptoms within the placenta group but not the placebo group, and reduced fatigue in placenta group participants at the end of the study compared to the placebo group.”
What is clear to me is that the answer to this question remains unclear! What is clear is that I don’t think it is wise to consume raw placenta due to the risks of bacterial contamination. Secondly, the levels of hormones left in the placental preparation and the most common preparation of steaming and drying leave hormone levels that are unlikely to influence much at all from a biochemical standpoint. It also seems that breastmilk production and neonatal weight gain aren’t influenced much by consumption of these pills.
The issue though in all of this is that while the previous research was of low quality, the current research while of better quality is at a low volume. These were pilot trials and not powered to find a difference likely. The finding in the subgroup of some effect on mood at the end of the study does leave some hope to those that believe in the power of the placenta to help. Would a larger study find benefit to this practice? My suspicion from a biochemical standpoint is not but that one may feel a benefit from a placebo response.
Should you go out and have your placenta prepared for consumption? If you have Kardashian like wealth then go for it if you think it will help. If you don’t then I would suggest waiting for something more definitive before spending your money on placentophagy.