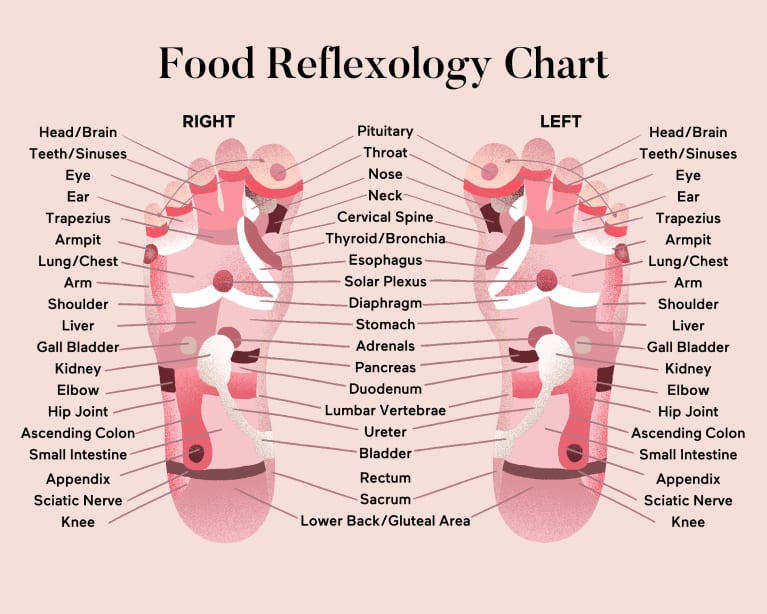
Every now and then something unconventional comes to my attention. Management of pain is something that I have written about before and have been a proponent of things such as kangaroo care and breastfeeding to help improve responses to pain from common procedures like heel lances. Foot reflexology is a practice that is based on the notion that there are pressure points on our bodies that if pressed can elicit internal reactions in our organs. A map of such points for the foot is shown below.
There are strong proponents of this practice and I have to admit I was taken once for a session myself as a gift from someone. At the very least I felt like it was a good massage although the pituitary point of my big toe was a little to painful as I recall to endure. Whether or not my pituitary health benefited from this I guess I will never know.
What about foot reflexology for heel lances in NICU?
This is the question that a Turkish group of researchers decided to look at in their paper The effect of foot reflexology on procedural pain before heel lancing in neonates. The authors used what they called a quasi-experimental design in which they took 30 healthy neonates and provided them with foot reflexology for 20 minutes prior to heel lance vs 30 neonates who just had the heel lancing without prior reflexology. These again were healthy term neonates with a BW from 2500-4000g who were all breastfed for up to 30 minutes before the heel lance. For the reflexology group they received 15-20 minutes of reflexology while being held in their mother’s arms. The Neonatal infant pain scale was used before, during and after the procedure and was interpreted by viewing videos of the neonates by two nurses blinded to the groups that the babies were in. Although the study was not randomized this step at least attempted to remove bias from the interpretation of the facial expressions.
Analyzing the Results
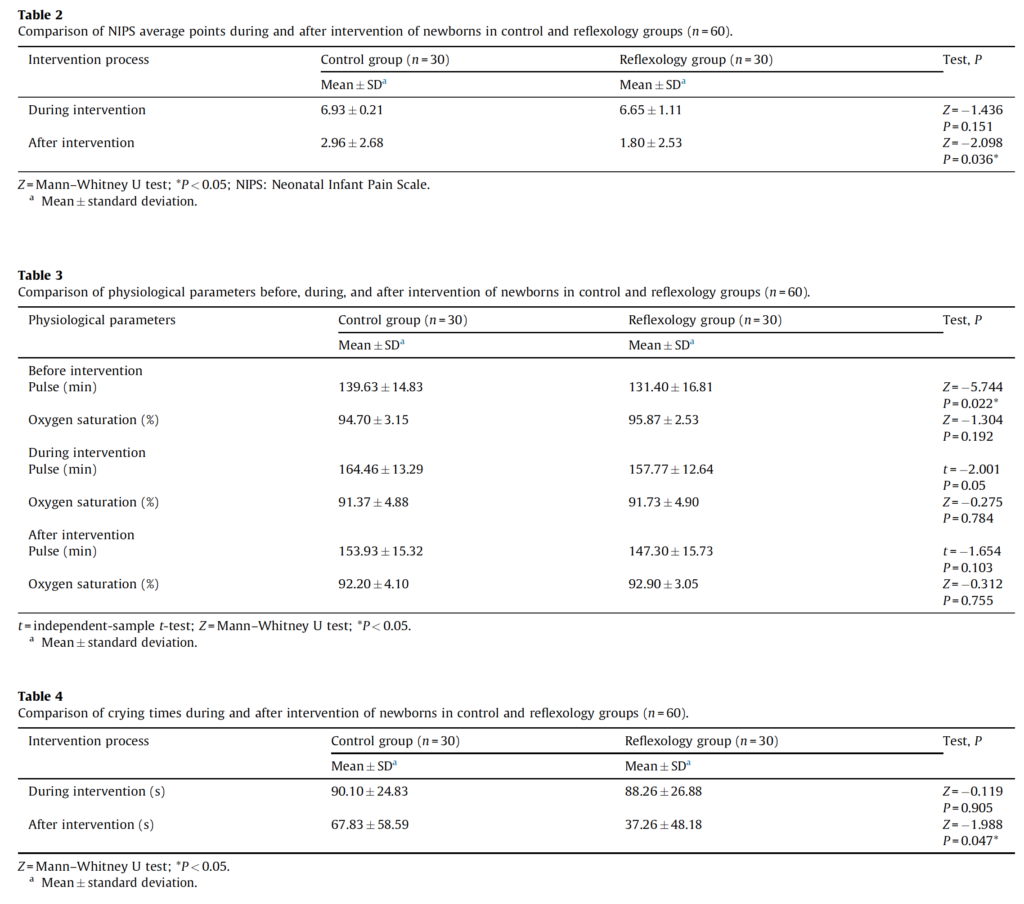
From the above tables there are a few things the authors would like your attention drawn to. The first is that during the heel lance the pain scores were the same but afterwards babies who had reflexology had lower pain scores that were significantly so. The issue though with this is the scores themselves since it is a difference that while statistically significant is of unlikely clinical impact. For the NIPS scores, a score over 3 is suggestive of pain. Given that the control arm is 2.96 and the reflexology 1.80 with wide confidence intervals I am not sure if we can say these babies were in a lot of pain. During the procedure which is when I would have hoped to see a difference in pain scores there is none and with scores close to 7 for both groups let’s not kid ourselves. These babies were in pain with and without reflexology.
Looking at physiological changes there were none that came out as significant although after the intervention as with the NIPS score the heart rates were a little lower in 154 vs 147 but again what clinical significance is this?
Interestingly, crying afterwards was much less and just reached significance but again is this real or just a fluke finding given how many things they have looked at?
Finally, the big issue I suppose I have here is that the control group was not held by the mother prior to the intervention as they were in the reflexology group. I think it would have given some strength to the study had mothers held their infant in the control group for 15-20 minutes prior to the heel lance. Not sure why that wasn’t done.
Ok, I am a skeptic. As you might suspect I think that the real intervention here was mother’s holding their infants for 20 minutes on average before the procedure. Having said that is a gentle massage of the foot such a bad thing? The authors are talking about a future RCT and I guess that could be done but I think there are better options out there such as kangaroo care, breastfeeding, drops of mother’s milk in the cheek or even just the scent of mother’s milk that are great options for reducing pain the neonate.
Will have a look though if an RCT does happen as I could always be wrong…
The Ortolani and Barlow manouvers are probably the two most requested parts of the physical exam that students ask to be shown. We line up several medical students who take turns applying the steps of abduction and then adduction, testing the stability of the hips. We routinely give oral sucrose, position in kangaroo care or breastfeed while performing other noxious stimuli such as heel lancing but at least in my centre give nothing for manipulating the hips in such a fashion.
How can we determine if a newborn feels pain?
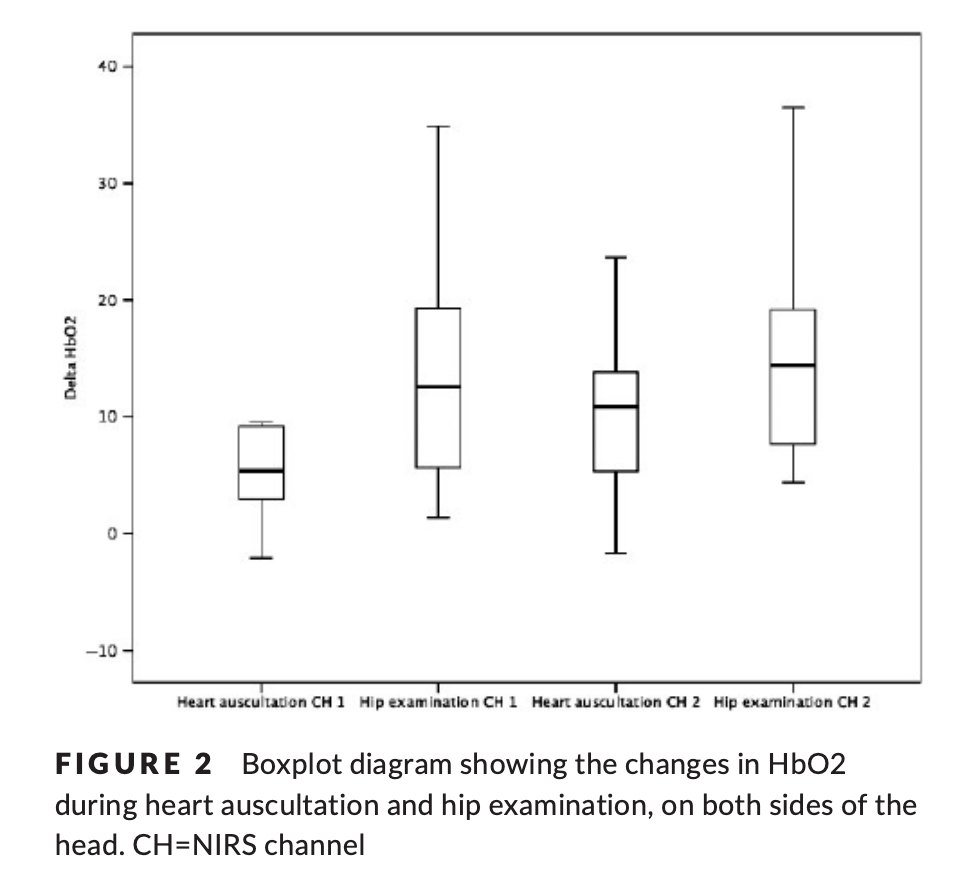
In a recent paper entitled Neurophysiological and behavioral measures of pain during neonatal hip examination by Pettersson M et al they used three methods to assess pain during the newborn hip exam. These were the Premature Infant Pain Profile‐Revised (PIPP‐R) scale which is generally used for such assessment as well as two relatively novel ways in the use of near‐infrared spectroscopy (NIRS) and galvanic skin response (GSR). In essence if the a region of the brain becomes more active during a painful experience more oxygen will be extracted during that time. By using auscultation of heart rate with a stethoscope as a control procedure which should not elicit pain the authors were able to compare in a controlled fashion 28 newborns undergoing both activities. The use of NIRS was previously demonstrated as valid in the paper Pain activates cortical areas in the preterm newborn brain. Galvanic skin response has also been demonstrated to correlate with pain and measures changes in skin conductance in the paper Skin conductance compared to a combined behavioural and physiological pain measure in newborn infants.
So the authors set out to compare findings in these 28 infants and standardized the study as much as they could by having one Neonatologist perform all hip exams and having a video recording of the infant’s face during the procedure assessed by two independent reviewers in order to assign the PIPP-R scores. While not a randomized trial, for the type of intervention being studied this was the right approach to take to determine the answer to their question.
The Findings
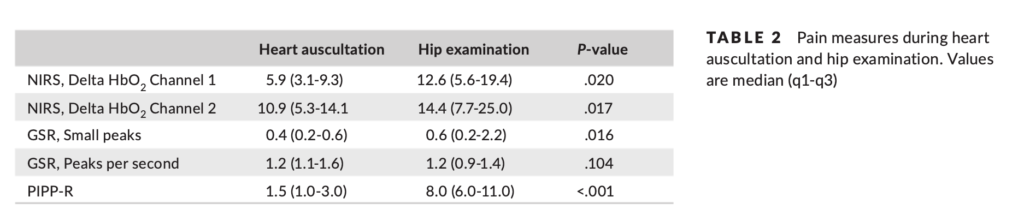
Interesting findings indeed. Statistically significant differences were noted in bilateral changes in oxygen extraction during hip examination as well as for the GSR small peaks. The PIPP-R scores as well were vastly different between the two groups suggesting that the areas of the brain responsible for perception of pain were indeed activated more so with manipulation of the hip than with auscultation of the heart.
What can we take from this?
The hip exam may elicit responses indicating pain but there remains the question of how much is actually elicited. Nonetheless, the authors findings are intriguing as they certainly challenge the notion that this is a quick exam that should be just done and gotten over with. Clearly bundling or Kangaroo Care are not an option here due to the nature of what is being done. The next time you are planning on doing such tests though should you at least consider non-nutritive sucking on a pacifier or sucrose solution if readily available? If not readily available then should it be?
I would consider myself fairly open minded when it comes to care in the NICU. I wouldn’t call myself a maverick or careless but I certainly am open to new techniques or technologies that may offer a better level of care for the babies in our unit. When it comes to “non-Western” concepts though such as therapeutic touch, chiropractic manipulations of infants and acupuncture (needle or otherwise) I have generally been a skeptic. I have written about such topics before with the most popular post being Laser acupuncture for neonatal abstinence syndrome. My conclusion there was that I was not a fan of the strategy but perhaps I could be more open to non traditional therapies.
Magnetic Acupuncture
This would appear to be the newest and perhaps strangest (to me at least) approach to pain relief that I have seen. I do love name of this study; the MAGNIFIC trial consisted of a pilot study on the use of auricular magnetic acupuncture to alleviate pain in the NICU from heel lances. The study was published in Acta Paediatrica this month; Magnetic Non-Invasive Acupuncture for Infant Comfort (MAGNIFIC) – A single-blinded randomized controlled pilot trial. The goal here was to measure pain scores using the PIPP scoring system for pain in the neonate before during and after a painful experience (heel lance) in the NICU. Being a pilot study it was small with only 20 needed per arm based on the power calculation to detect a 20% difference in scores. The intervention used small magnets placed at specific locations on the ear of the infant at least two hours before the heel lance was to occur. Before I get into the results, the authors of the study provide references to explain how the therapy works. Looking at the references I have to admit I was not able to obtain complete papers but the evidence is generally it would appear from adult patients. The explanation has to do with the magnetic field increasing blood flow to the area the magnet is applied to and in addition another reference suggests that there are affects the orbitofrontal and limbic regions which then impacts neurohormonal responses as seen in functional MRI. The evidence to support this is I would have thought would be pretty sparse but I was surprised to find a literature review on the subject that looked at 42 studies on the topic. The finding was that 88% of the studies reported a therapeutic effect. The conclusion though of the review was that the quality of the included studies was a bit sketchy for the most part so was not able to find that this should be a recommended therapy.
So what were the results?
Despite my clear skepticism what this study did well was that aside from the magnets, the intervention was the same. Twenty one babies received the magnetic treatments vs 19 placebo. There was a difference in the gestational ages of the babies with the magnet treated infants being about two weeks older (35 vs 33 weeks). What difference that might in and of itself have on the PIPPs scoring I am not sure. The stickers were applied to the ears with and without magnets in a randomized fashion and the nurses instructed to score them using the PIPP scoring system. Interestingly, as per their unit policy all babies received sucrose as well before the intervention of a heel lance so I suppose the information gleaned here would be the use of magnets as an adjunctive treatment. No difference was noted in the two groups before and after the heel lance but during the procedure the magnet treated infants had a difference in means (SD): 5.9 (3.7) v 8.3 (4.7), p=0.04). No differences were found in secondary measures such as HR or saturation and no adverse effects were noted. The authors conclusions were that it was feasible and appears safe and as with most pilot studies warrants further larger studies to verify the results.
Should we run out and buy it?
One of the issues I have with the study is that in the introduction they mention that this treatment might be useful where kangaroo care (KC) is not such as a critically ill infant. Having placed infants who are quite sick in KC and watched wonderful stability arise I am not sure if the unit in question under utilizes this important modality for comfort.
The second and perhaps biggest issue I have here is that although the primary outcome was reached it does seem that there was some fishing going on here. By that I mean there were three PIPP scores examined (before, during and after) and one barely reached statistical significance. My hunch is that indeed this was reached by chance rather than it being a real difference.
The last concern is that while the intervention was done in a blinded and randomized fashion, the evidence supporting the use of this in the first place is not strong. Taking this into account and adding the previous concern in as well and I have strong doubts that this is indeed “for real”. I doubt this will be the last we will hear about it and while my skepticism continues I have to admit if a larger study is produced I will be willing and interested to read it.
As those of you who have been following this blog are aware, I am always on the lookout for strategies that can help minimize blood work without sacrificing care in the NICU. At particular risk our the very premature infants in our units who for example at 1 kg have about 80-90 mL of blood. It does not take very many 0.5 – 1 mL “small” draws to create anemia. In a recent study (free article in link) of infants less than 1500g entitled A mathematical modeling approach to quantify the role of phlebotomy losses and need for transfusions in neonatal anemia, the authors studied 26 infants over a one month period. The results were staggering in that these infants experienced 138 +/- 21 blood draws with an average of nearly four transfusions per patient. While the authors do not specify what type of testing was done they did find a shocking statistic that 59% of the blood collected by weight of sample was discarded. This certainly stresses the point that we should aim to minimize the volume of sample collected in each case to that which is only necessary for the equipment to run. Furthermore, strategies to minimize sample draws should be utilized where possible and if accuracy permits point of care technology may further reduce volumes required and provide immediate results at the bedside. Lastly where possible, utilizing non-invasive technology to avoid blood draws needs to be explored when possible and was the subject of another post on Masimo non-invasive HgB measurement (http://wp.me/p5NWfD-1t).
Certainly in sick neonates whether they be term or preterm the drawing of blood gases to monitor ventilation contributes to the anemia of prematurity which often culminates in a transfusion. Sicker infants with greater lability due to respiratory compromise are deserving of optimal ventilation and this is achieved by monitoring pCO2 levels in arterial or venous samples. There have been different strategies employed to replace the sampling of CO2 by blood gas analysis which have not been very successful but there is one that I believe has promise that I will discuss at the end.
Transcutaneous pCO2 measurement was introduced in the 1980s. While this technology does allow measurement of pCO2 the variation between true arterial pCO2 and tcPCO2 can be wide making the technology difficult to implement on a consistent basis. In particular the accuracy in infants <28 weeks has been quite poor leading to increased numbers of arterial and venous samples to “check” ow closely the results correlate. As was described in 2005 by Aliwalas LL et al the technology in this group who actually have the highest number of blood draws does not meet the required standard to replace arterial pCO2 measurements (http://www.ncbi.nlm.nih.gov/pubmed/15496874)
Another method is of directly sampling exhaled CO2 in ventilated patients. Traditionally such measurements were taken with proximal gas sampling and in neonates in particular the results were discouraging. Problems encountered with proximal end tidal sampling were related to the lack of cuffed endotracheal tubes in part as the measured gas would be diluted with air in the presence of any leak around the tube leading to underestimation of true CO2 levels. Furthermore, in the presence of significant pulmonary disease the clearance of CO2 may be impaired such that the arterial pCO2 – ETCO2 difference may be quite large. For a review see the free article by Malloy and Deakins Are carbon dioxide detectors useful in neonates? The agreement between arterial and proximal sampling measured in this way has been quite variable and as such the technology has not really caught on to any great degree for monitoring ventilated infants. That being said it can be quite useful at determining if the endotracheal tube is in the trachea or esophagus. The presence of the waveform even if not yielding an accurate level confirms proper placement although where the tube sits in the trachea still needs confirmation.
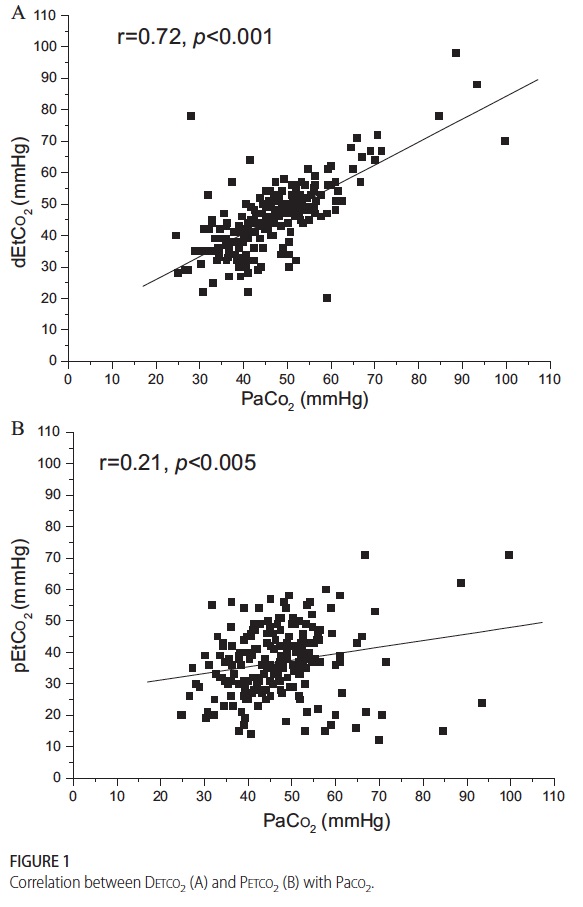
The final method for sampling CO2 is the one which I believe holds the most promise for actually reducing blood draws and by extension risk of anemia and pain in the neonate. Kugelman and colleagues in Haifa, Israel published the following paper (free article in the link) A novel method of distal end-tidal CO2 capnography in intubated infants- comparison with arterial CO2 and with proximal mainstream end-tidal CO2. This creative study utilized a double lumen endotracheal tube which had been designed for surfactant installation and distal pressure measurement to instead sample pCO2 near the carina. This strategy was postulated to eliminate the issue with dilution of gas from proximal sampling and provide a closer measurement of true pCO2 when compared to arterial CO2 and proximal sampling. They studied 27 infants with varying degrees of pulmonary condition severity although most had RDS. When comparing the three methods of pCO2 measurement the following was found.
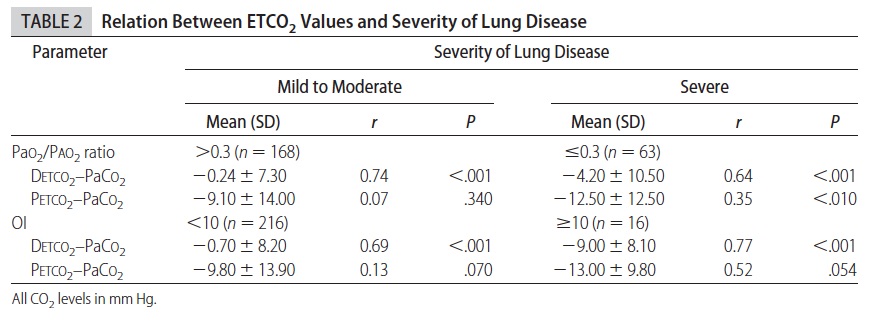
This demonstrates that while proximal measurement was quite poorly correlated with true arterial pCO2 the distal measurement was much more accurate. In fact the mean differences between arterial pCO2 and distal measurement was -1.5 mm Hg while that of proximal measurement -10.2 mm Hg albeit with wide confidence intervals. As found in other studies of proximal end tidal CO2 measurement, worse pulmonary disease correlated with worse accuracy as shown in table 2.
As the pCO2 rises above 60 the accuracy is less but remains much better than proximal measurements. Interestingly the same group has published an additional trial using high frequency ventilation and confirmed the measurements remain accurate. (http://www.ncbi.nlm.nih.gov/pubmed/22328495)
So what does the future hold? in VLBW infants one concern may be the internal diameter of the smallest double lumen tubes and the effect of upsizing to a larger tube and risk of subglottic stenosis. After a personal communication with Dr. Kugelman I understand that this has not been an issue in their unit as they tend to use these double lumen tubes in most if not all of the their infants. The accuracy is sufficient enough from my point of view that units should be able to implement this strategy at least in larger infants at first (those who would need a 3.0 ETT and larger) to see the effect on blood sampling. I suspect that one blood gas a day to determine accuracy in a given patient would be sufficient most of the time if the numbers were found to correlate well.
I would welcome feedback from people who work in units where this strategy has been utilized. How effective is it? Did it reduce your blood gas draws or increase them due to unreliability? Have you seen a rise in subglottic stenosis? Please send your feedback to either this site or at my Facebook page at www.facebook.com/AllThingsNeonatal.




 This demonstrates that while proximal measurement was quite poorly correlated with true arterial pCO2 the distal measurement was much more accurate. In fact the mean differences between arterial pCO2 and distal measurement was -1.5 mm Hg while that of proximal measurement -10.2 mm Hg albeit with wide confidence intervals. As found in other studies of proximal end tidal CO2 measurement, worse pulmonary disease correlated with worse accuracy as shown in table 2.
This demonstrates that while proximal measurement was quite poorly correlated with true arterial pCO2 the distal measurement was much more accurate. In fact the mean differences between arterial pCO2 and distal measurement was -1.5 mm Hg while that of proximal measurement -10.2 mm Hg albeit with wide confidence intervals. As found in other studies of proximal end tidal CO2 measurement, worse pulmonary disease correlated with worse accuracy as shown in table 2.