If you work in NICU you will have seen many babies who have passed through the stages of apnea, weaned off respiratory support and have reached a sufficient weight for discharge but alas will just not feed. Different strategies have been employed to get these infants feeding that rely in many cases on a cue based approach but in the end there are some that just won’t or can’t do it. Many of these babies will be sent home either with NG feedings or if it appears to be a more long term situation a gastrostomy tube. For this blog post I am going to present to you some novel research that suggests there may be another way to approach this and would like to thank one of the followers of my social media for alerting me to this work. You know who you are as the saying goes!
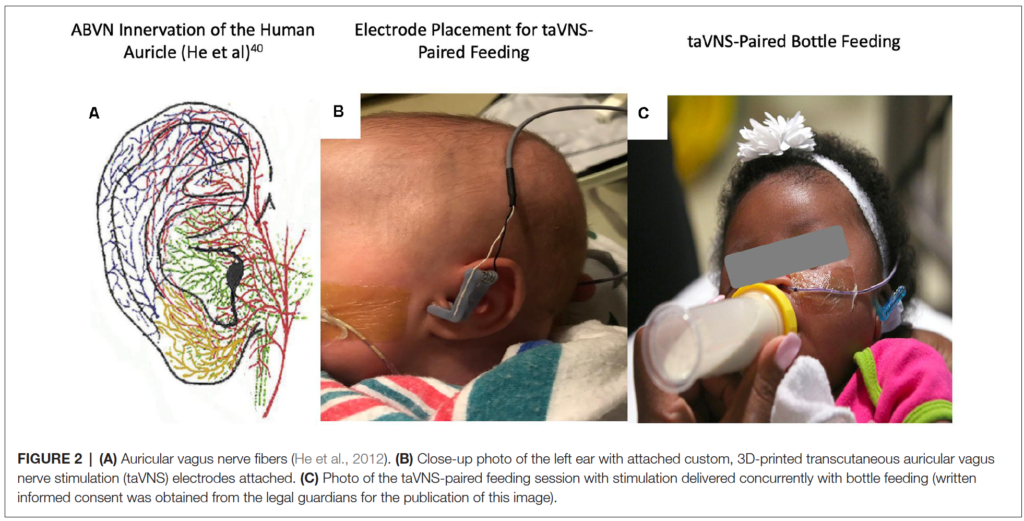
This was an open label Phase 0 trial (few patients as a pilot) using taVNS to help improve feeding in ex-preterm or 3 recovering from HIE infants who were now past term and all headed towards a gastrostomy tube. The hospital carrying out the study entitled Transcutaneous Auricular Vagus Nerve Stimulation-Paired Rehabilitation for Oromotor Feeding Problems in Newborns: An Open-Label Pilot Study by Badran BW et al did not come out of thin air. Prior research in adult patients recovering from stroke found in multiple studies (all referenced in the paper) that motor stimulation accompanied by VNS improves motor function recovery. The objective here then was to see if stimulation of the auricular nerve along with assessment and motor treatments from an occupational therapist once a day could help improve feeding and avoid GT placement. The trial overview is as shown below.
The centre in which the study was done had a historical rate in this population of <10% of such patients avoiding a GT (all reaching term equivalent age and not showing an improvement in feeds). This was demonstrated in previous work by at the Medical University of South Carolina (MUSC). “Preterm infants who have not reached full PO feeds by 40-week gestational age (GA) and/or after 40 days of attempting PO feeds have a >90% chance of eventually needing G-tube implantation to achieve full enteral feeds (Ryan and Gehle, 2019).”
The Intervention
taVNS was done once a day during a bottle feed and timed with observed suckling and swallowing by an OT. The stimulation was stopped during a pause in feeding.
As you read this you may be concerned about side effects (as I was) of passing an electrical current to the ear and stimulating the auricular branch of the vagus nerve. This has been shown in other work to activate both afferent and efferent pathways of the vagus nerve and enhance plasticity and functional motor recovery. Could you then apply the same to improving development of the motor pathways of the preterm newborn or patient recovering from HIE? The authors examined skin irritation, pain scores and incidence of bradycardia before and during feeding while stimulation was occurring and found no difference in any of the measures. In order to minimize pain the authors increased the current by 0.1 mA until they perceived stimulation by change in facial expression, shrugging or fidgety movements. In the event of an increase in pain scoring by 3 the dose was decreased by the same amount. in the end the intervention was deemed safe without any adverse effects.
The primary outcome was ability to increase and maintain full daily PO intake for 4 days (>120 mL/kg/d and maintain a weight gain of >20 g/day until discharge.
Why you should care about the results
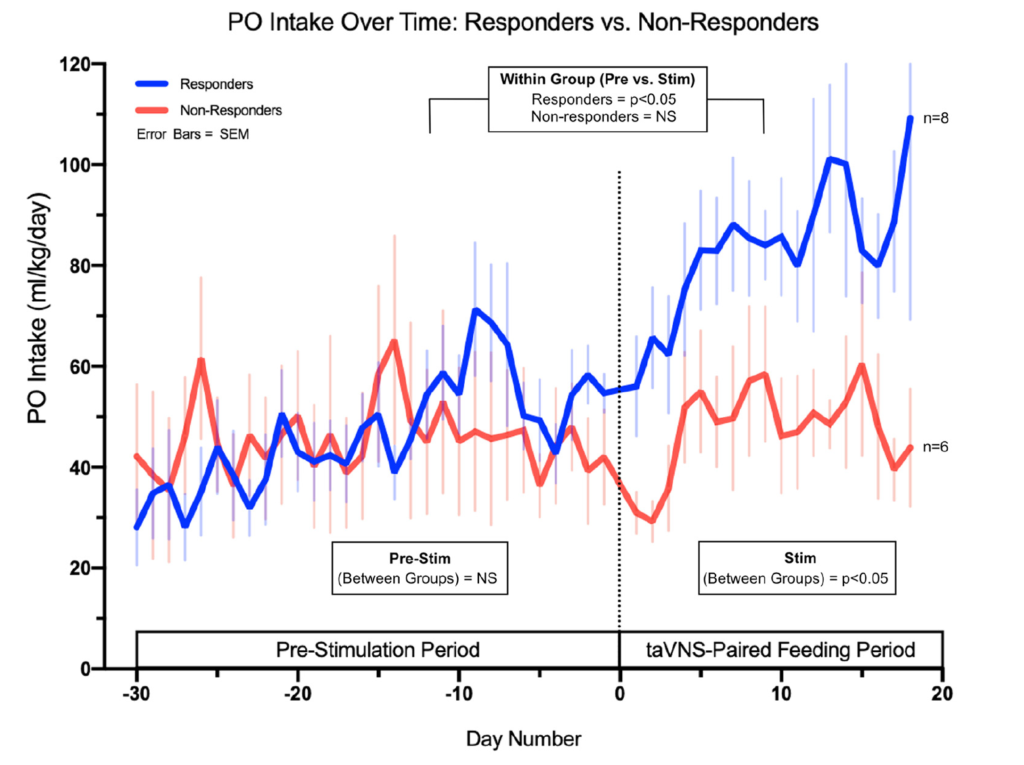
If you work in a hospital like mine you would probably find that once the discussion about a GT placement begins, few miraculously avoid it. In this study they found that 8 of the 14 patients or 57% avoided the GT. Their historical achievement in this regard was <10%. This could be by chance of course since the study is a small one but when looking at the PO intake between non-responders and responders they demonstrate the following.
The authors found no statistically significant increase in the non-responders after the taVNS in PO feeds but also note there were three infants born to mothers with diabetes in this group. I have commented before on the effect of diabetes on successful feeding so this certainly could have affected the success of this group. If you look at the change over time in the responder group they look graphically like there was an upwards trend in the feeding ability prior to the intervention although the increase or slope of the improvement due to small numbers was not significant. The takeoff in feeding afterwards was.
The findings in this study are extremely exciting to me. As units across the globe struggle with patient flow, one of the most common reasons for these patients to stay in hospital is no longer BPD or apnea but inability to feed. The idea that such a simple intervention that is done once daily for 30 minutes might influence the development of feeding coordination in these at risk infants is phenomenal in terms of its impact on patient flow.
If you wonder about whether this is a one off study, there is a lot of active research in this area. A quick search of clinicaltrials.gov uncovers 61 studies on taVNS recruiting at the moment for a variety of ailments. In fact the next study is a Phase 1 trial aiming to recruit 40 patients and is underway. If interested the link to the study is here.
This could turn into a book one day I suppose but I have become interested in chalenging some of my long held beliefs these days. Recently I had the honour of presenting a webinar on “Dogmas of Neonatology” for the Indian Academy of Pediatrics which examined a few practices that I have called into question (which you can watch in link). Today I turn my attention to a practice that I have been following for at least twenty years. I have to also admit it is something I have never really questioned until now! In our institution and I suspect many others, infants born under 1250g have been fed every two hours while those above every three. The rationale for this has been that a two hour volume is smaller and causes less gastric distention. This in theory would benefit these small infants by helping to not compromise ventilation or lead to reflux. Overwhelming the intestine with large distending boluses would also in theory lead to less necrotizing enterocolitis. All of this of course has been theoretical and I can thank those who preceded me in Neonatology for coming up with these rules!
Study Challenges This Old Belief
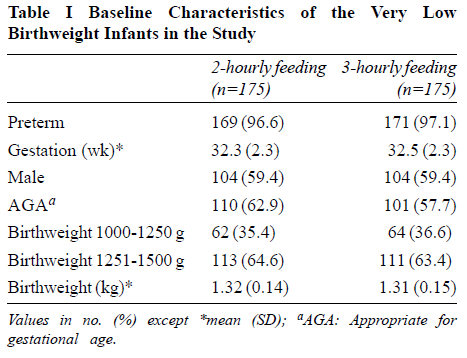
Yadav A et al published Two-hourly versus Three-hourly Feeding in Very Low Birthweight Neonates: A Randomized Controlled Trial out of India (well timed given my recent talk!). The authors randomized 175 babies born between 1000-1500g to either be fed q2h vs q3h once they began protocol feeding. The primary outcome was time to full feedings. Curiously, the paper indicates they decided to do a preplanned subgroup analysis of the 1000-1250 and 1251 -1500g groups but in the discussion it sounds like this is going to be done as a separate paper so we don’t have that data here.
The study controlled conditions for determining feeding intolerance fairly well. As per the authors:
“Full enteral feed was defined as 150 mL/Kg/day of enteral feeds, hypoglycaemia was defined as blood glucose concentration <45mg/dL [15]. Feed intolerance was defined as abdominal distension (abdominal girth ≥2 cm), with blood or bile stained aspirates or vomiting or pre-feed gastric residual volume more than 50% of feed volume; the latter checked only once feeds reached 5 mL/kg volume [16]. NEC was defined as per the modified Bells staging.”
We don’t use gastric residuals in our unit to guide cessation of feedings anymore but the groups both had residuals treated the same way so that is different but not somethign that I think would invalidate the study. The patients in the study had the baseline characteristics shown below and were comparable.
Results
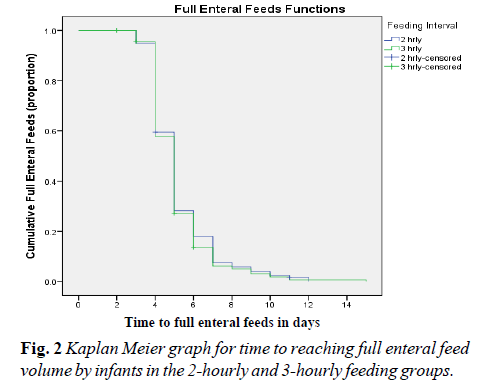
It will be little surprise to you that the results indicate no difference in time to full feedings as shown in Figure 2 from the paper.
The curves for feeding advancement are essentially superimposed. Feeding every two vs three hours made no difference whatsoever. Looking at secondary outcomes there were no differences as well in rates of NEC or hypoglycemia. Importantly when examining rates of feeding intolerance 7.4% of babies in the 2 hour and 6.9% in the 3 hour groups had this issue with no difference in risk observed.
Taking the results as they are from this study there doens’t seem to be much basis for drawing the line at 1250g although it would still be nice to see the preplanned subgroup analysis to see if there were any concerns in the 1000-1250 group.
Supporting this study though is a large systematic review by Dr. A. Razak (whom I have collaborated with before). In his systematic review Two-hourly versus three-hourly feeding in very low-birth-weight infants: A systematic review and metaanalysis. he concluded there was no difference in time to full feeds but did note a positive benefit of q3h feeding in the 962 pooled infants with infants fed 3-hourly regainin birth weight earlier than infants fed 2-hourly (3 RCTs; 350 participants; mean difference [95% confidence interval] -1.12 [-2.16 to -0.08]; I2 = 0%; p = 0.04). This new study is a large one and will certainly strengthen the evidence from these smaller pooled studies.
Final Thoughts
The practice of switching to q2h feedings under 1250g is certainly being challenged. The question will be whether the mental barriers to changing this practice can be broken. There are many people that will read this and think “if it’s not broken don’t fix it” or resist change due to change itself. The evidence that is out there though I would submit should cause us all to think about this aspect of our practice. I will!
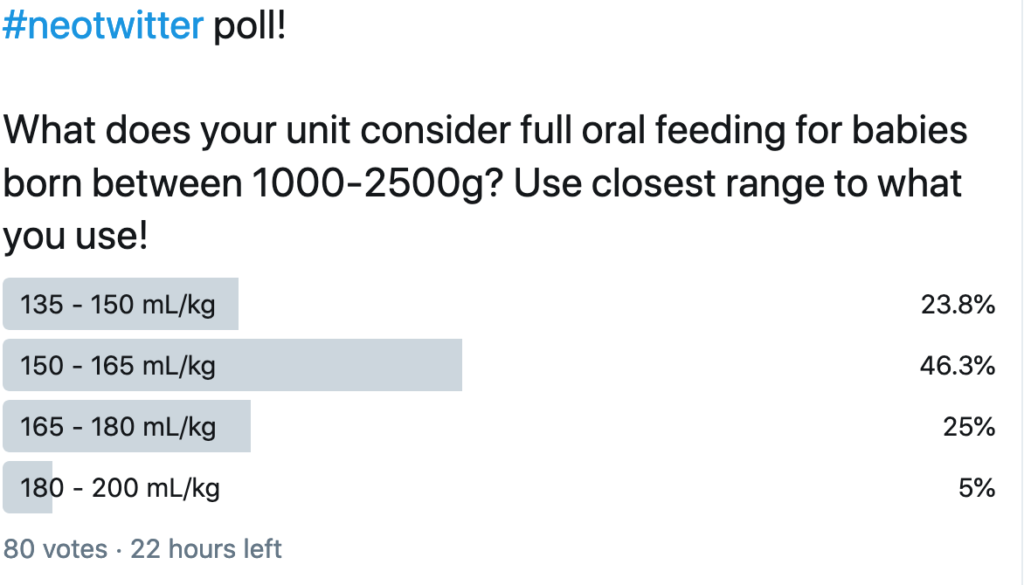
Since the dawn of my time in Neonatology there has been cibophobia! What is this you ask? It is the fear of food and with some flexibility in the definition I would apply this to large volumes of milk rather than the fear of food itself. Most units in the world seem to use a volume range of about 135 – 165 mL/kg/d as a range considered to mean “at full feeds”. As I was discussing this on rounds today I was quick to point out though that babies with neonatal opioid withdrawal syndrome (NOWS) frequently take in excess of 200 mL/kg/d and we don’t worry about it. The counter argument though is that these infants are “bigger” and should be able to tolerate a larger volume. As readers of this blog know I truly enjoy coming across papers that suggest a change to something considered dogma. Today is one of those days as I am choosing to explore in more depth an abstract that I posted to Twitter and Facebook last month.
On the day of this blog release I also took a poll on Twitter and found some interesting results that make this post all the more important to share. Take a look!
Are Bigger Volumes Better?
Travers CP et al chose to challenge this long held practice in their recent paper Higher or Usual Volume Feedings in Very Preterm Infants: A Randomized Clinical Trial. It was a simple yet wonderful trial that asked the question of whether for infants < 32 weeks GA at birth with BW from 1000-2500g would higher volume feedings of 180-200 vs 140-160 ml/kg/d help increase growth velocity. Randomization occurred after infants had reached 120 mL/kg/d of oral feedings. In both arms advancements from this point were the same and fortification occurrred as per usual practrice but in each arm strategies targeted individual fortification to weight gain.
The authors were seeking a 3 g/kg/d difference in growth and needed 224 infants to demonstrate this difference. They enrolled the same at a mean GA of 30.5 weeks and a BW of 1445 grams. Birth characteristics including gestational age, weight, sex, race/ethnicity, Apgar scores, head circumference, length, and proportion of infants with a weight <10th percentile at birth did not differ between groups.
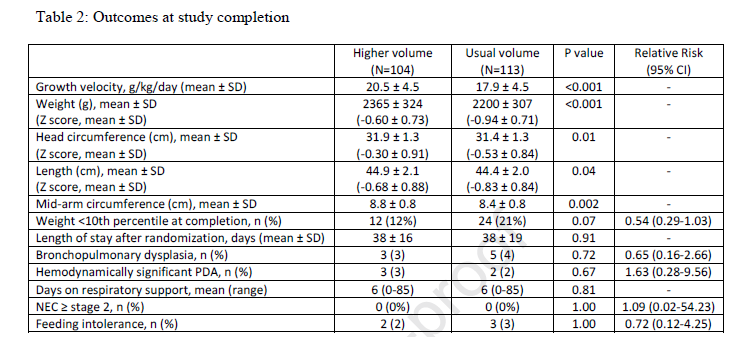
The outcomes showed differences as shown below.
Looking at the results
All in all I would say the results are a smashing success. Growth velocity was improved and not just in weight but in head circumference and length. What I find interesting is that if fortification of milk was targeted regardless of the volume used I am a bit baffled as to why the growth rate would still be better but it was. The difference in caloric intake received between groups was approximately 9 kcal/kg/day at day 7 after study entry (126 kcal/kg/day versus 117 kcal/kg/day) and 16 kcal/kg/day from day 14 after study entry onwards (139 kcal/kg/day versus 123 kcal/kg/day).
Blinding here would have been a challenge as nurses and other health care providers would have been able to calculate the expected volumes at different fluid administration levels. Nonetheless there was a difference.
The question though that many would ask is whether this better growth came at the expense of greater morbidity. Let’s be clear here that the study was not powered to look at adverse outcomes and the numbers in the above table are small but no difference was seen nonetheless. To appease the most cautious of Neonatologists I suspect a larger study powered to look at adverse outcomes will be needed. What this study does though is raise the question of whether we can and should try larger volumes. As the title suggests I wonder about getting bigger faster so one can go home. With this more rapid rate of growth can we expect a faster maturation as well? I doubt it but it is something to certainly question in a larger study!
I presented this topic as a fellow many years ago after a paper came on the scene suggesting better outcomes with a faster approach. The paper Randomized trial of “slow” versus “fast” feed advancements on the incidence of necrotizing enterocolitis in very low birth weight infants. was plagued by the same issue as others created around those years which was a small number of patients at the lowest gestational ages. Any differences in sub analyses were difficult to really believe as the outcomes could have easily been explained by chance. Having said that, many centres began advancing feeds a little faster than the typical 20 ml/kg/d in favour of 30 ml/kg/d. It would take some time to coordinate a trial large enough to really answer questions about relevant issues such as time to developmental outcomes, time to full feedings and rates of NEC and the time appears to be now.
The SIFT trial
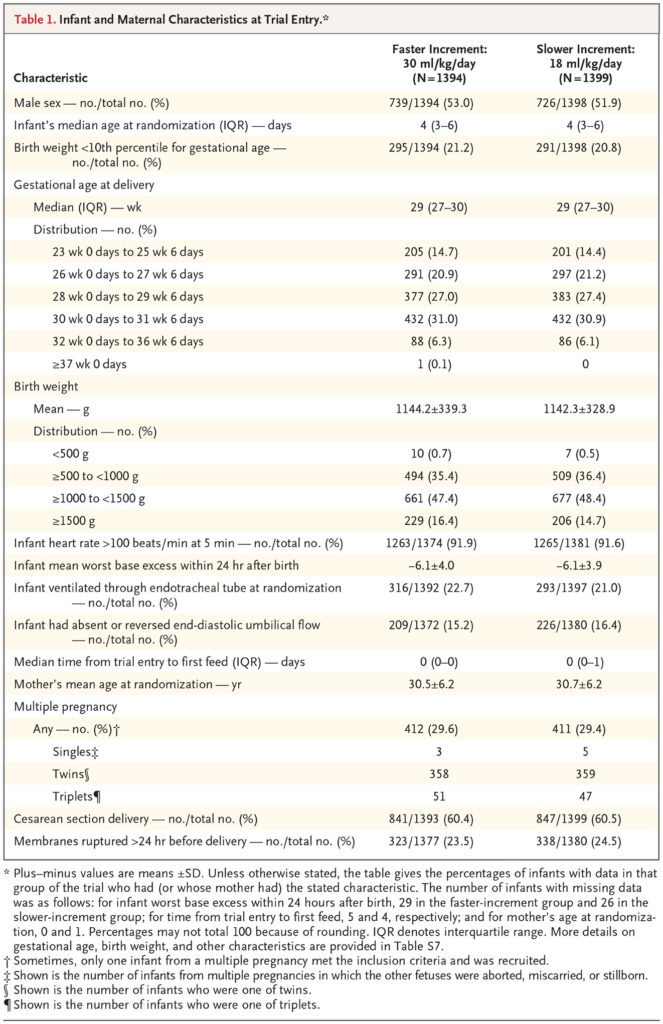
This trial (Controlled Trial of Two Incremental Milk-Feeding Rates in Preterm Infants) was the result of a great deal of coordination between 55 different centres. For inclusion, infants had to be <1500g and <32 weeks gestational age at birth. Once the decision was made to advance feeds, babies were randomized to receive increases of 18 mL/kg/d vs 30 ml/kg/d. The primary outcome was survival without mod-erate or severe neurodevelopmental disability at 24 months CGA. What is striking about the study is its size. The number of babies in the fast arm was 1394 while 1399 in the slower group. In terms of having sufficient numbers of infants who were at the earliest gestational ages they were able to accomplish this as shown in this table.
Importantly when looking at the primary outcome 87.4% of infants in the faster group vs 88.7% in the slower group were followed up for assessment. It is also worth mentioning that this is even more impressive in terms of retention when one considers that about 6% in both arms died before assessment.
What were the findings then?
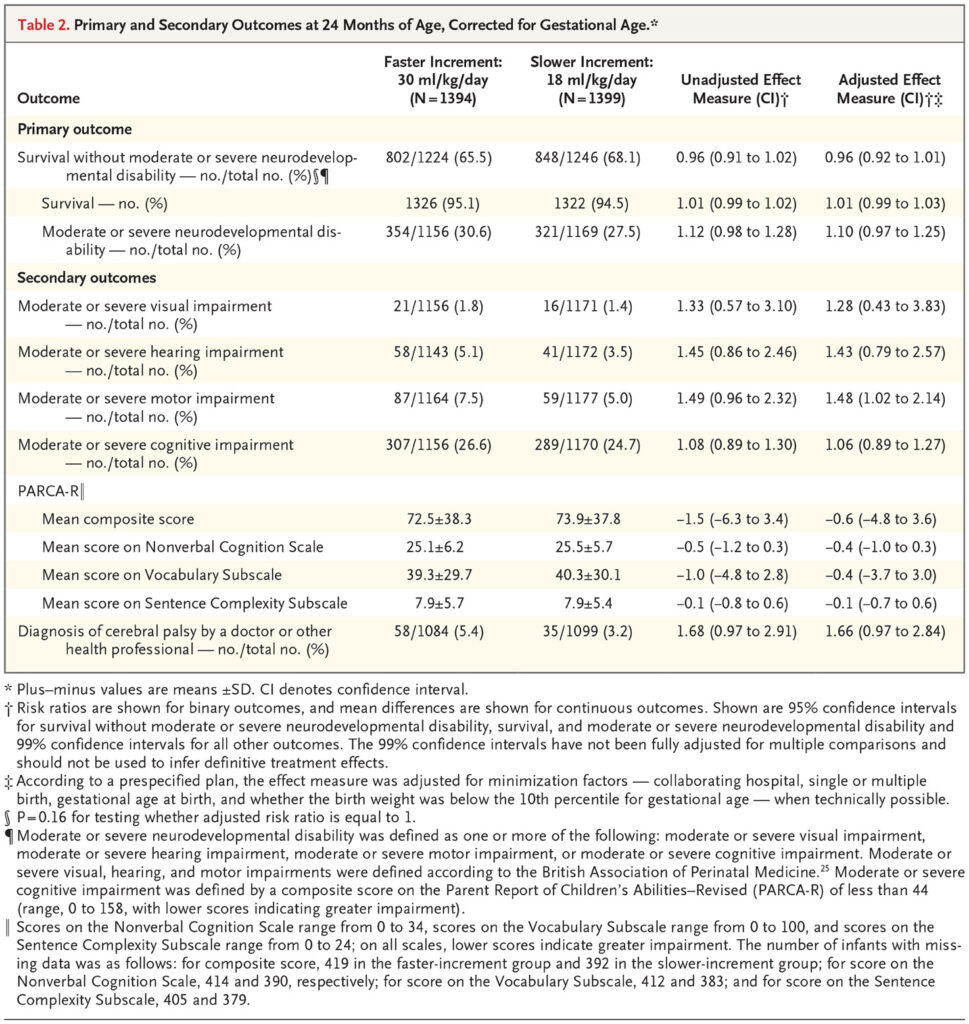
There was no difference in the primary outcome or for that matter each of its’ competing parts.
The authors in a secondary analysis did show a very marginal significant finding favouring slow feeds with respect to motor outcome. I concur with the authors though that given the small effect size and the “fishing” for results this likely is simply a chance finding. I can’t think of any reason why that would be the case either from a biological standpoint.
Not surprisingly another significant finding was shorter durations to reach full feeds (10 vs 7 days) and days on TPN at 11 vs 9 in the slow vs fast groups. In spite of having less need for central venous access, the authors were unable to show a reductoin in late onset sepsis or NEC.
Does it change your management?
I suppose that depends on what your management currently is. If you are like our centre and already advancing feedings by 30 ml/kg/d then I suspect not much. If you are in a slow centre one can take away from this study that at the very least you can lessen your patient’s need for central venous access and TPN. Based on this study and my suspicion that there will be no bigger trial forthcoming, whatever you decide to do this is about the best data that you will be getting.