Who doesn’t love a good match up?! Supporting neonates in need of resuscitation after delivery has been the subject of many studies over the years. The movement has certainly been to non-invasive support with CPAP or NIPPV but some babies need some degree of support with PPV after delivery when they simply won’t breathe. Prior to intubation the rise of the t-piece resuscitator has meant that practitioners can set a PIP and PEEP and with only a finger press to deliver a tidal volume at set pressure and with the finger released provide CPAP through the same device. The only problem potentially with use of these devices is the imposed work of breathing (iWOB) which has been measured in other studies. Any device I have used has provided ventilation through a mask so imagine my surprise to come across a new device called rPAP using prongs from the original infant flow design. From the manufacturers website the company claims that their design used with either a mask or nasal prongs reduces iWOB by 92% compared to other comparable machines! Imagine my greater surprise to see a head to head RCT comparing this new device to standard t-piece resuscitators with a mask.
The intervention was completed with one of three outcomes were met.
Infant intubated
Stable and breathing on method of support after a minimum of 10 minutes of support.
At 30 minutes when respiratory support could continue as decided by the clinician without crossover allowed.
Looking at the appendices for the trial it appears that one could use either device to administer PPV or CPAP but the point of the trial was that the devices would be used to support the infants until one of the three above criteria were met. If the claims about reduced iWOB were true compared to other devices in use then one might expect to see a difference in the primary outcome of incidence of intubation or death within 30 minutes of birth.
In total there were 250 infants recruited with 127 assigned to the rPAP and the other 123 to t-piece resuscitation. The mean GA in the trial was 24.8 weeks and the baseline characteristics between groups were similar although the group randomized to the rPAP has more c-sections and more general anesthetic exposure compared to the t-piece group. Lastly, humidification of gases during resuscitation was similar between the two groups.
How Did They Compare?
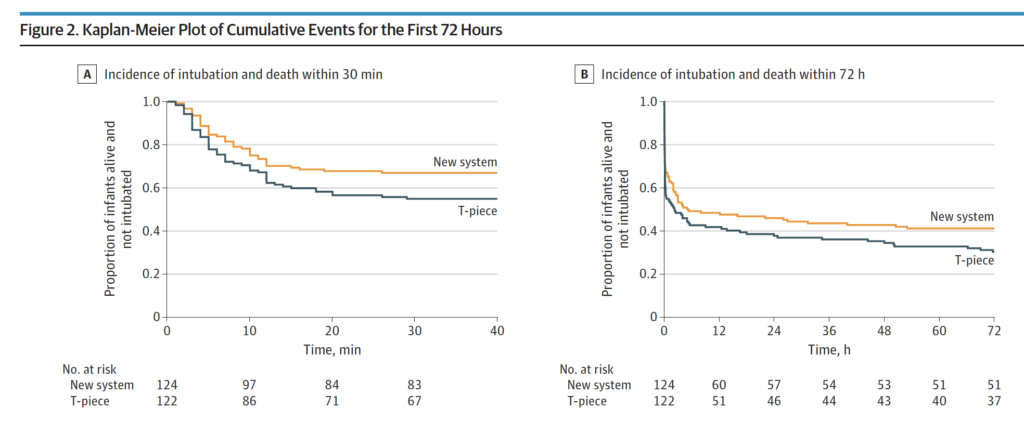
It just might be that the claims of decreased iWOB might have merit. In Figure 2 below the Kaplan-Meier curves show a difference favouring the rPAP device when looking at the primary outcome. This difference was significant with 41 of 124 infants (33.1%) in the rPAP group and in 55 of 122 infants (45.1%) in the T-piece group having the primary outcome of intubation or death within the first 30 minutes of life. Moreover when looking at the adjusted odds ratio it was still significant at 0.53; 95% CI, 0.30-0.94. The incidence of intubation and death in the first 72 hours although trending towards favouring the new system did not reach statistical significance.
Finally, none of the secondary outcomes reached statistical significance which included such things as death in the delivery room, use of surfactant, or PPV in the DR.
Does it make sense?
If you had asked me to tell you prior to the study whether resuscitation with nasal prongs vs a mask would be different I would have said a mask would be better due to less leak. Turns out based on this data that I would be wrong in that guess. A look at the website though for the rPAP device indicates that it can be used with a mask or nasal prongs. It would have been nice in the study presented here to have used a mask as a third arm with the rPAP device as it leaves me wondering a bit whether it was the interface that mattered more than the type of driver used? Maybe I am wrong and by using prongs it allows the infant to have less iWOB than with a mask over the mouth and nose? Could it be that it has more to do with that that the type of driver whether it is a traditional t-piece resuscitator or the new rPAP device? Regardless, I have a suspicion that these results will resonate with people. A posting of the abstract alone has garnered a lot of attention on twitter this week so clearly this is of interest.
I don’t think there is much fault to find in this study other than my question of why they didn’t choose to have a head to head comparison with masks as well but perhaps that is for another study. I imagine we will see this approach adopted in many centres around the world as they replace their traditional t-piece resuscitators in need of replacement. I also suspect there will be many that will want a larger study before adopting this strategy to look more closely with come faith in the results at secondary outcomes in particular having to do with safety.
One thing is for certain. There will be more studies to come!
If there is a country that leads this site in terms of mentions it has to be Sweden. This isn’t just because I happen to know some Neonatologists from there who are fine people but because of the fantastic research that spills forth from their national registry of births. Surfactant is one of the oldest treatments we have in Neonatology and we know that in babies with RDS giving it early within 2 hours has benefits such as reduction in pneumothorax. The reality though is that as we have become familiar with the therapy its use has spilled over to other conditions. Years ago use of surfactant in meconium aspiration syndrome was shown to reduce need for ECMO. It has also been shown to imrove clinical condition in babies with pneumonia. Interestingly as a fellow I was criticised one call night for wanting to give a three day old baby with a history of RDS and high FiO2 requirements a repeat dose of surfactant. That was in 2001 and at that time no one could believe I was suggesting such an odd thing to give a dose after 48 hours yet now this is commonplace. Again as we have become more comfortable with surfactant such “off label” use spreads. I am not being critical of my colleagues back in 2001 as that was what the “conventional wisdom” was with respect to surfactant but that was then and this is now.
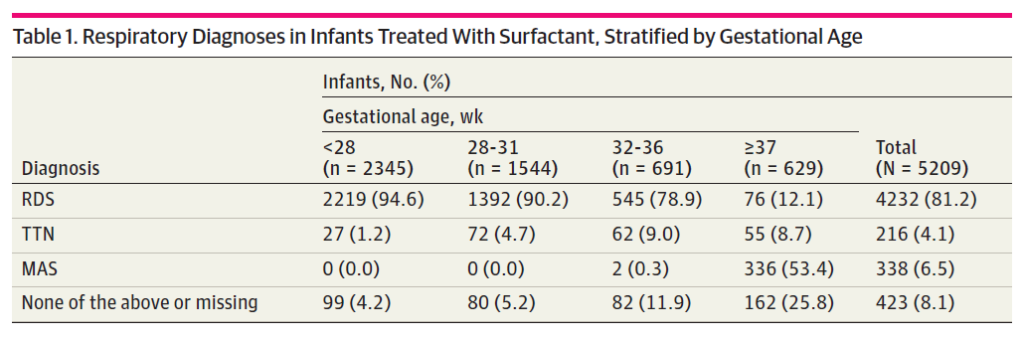
Looking at their registry data for 97377 infants born from 2009-2018 they found 7980 surfactant administrations to 5209 infants. The reasons for surfactant administration are shown in the table 1 below from the paper. Clearly and not surprisingly the bulk of surfactant administration is for RDS especially as gestational age declines. Given that so few preterm infants will pass meconium in-utero it also is understandable why MAS clusters in the more mature babies.
When it comes to multiple surfactant administrations they found 59.2% received 1 administration, 25.8% received 2, 7.3% had 3, and 2.8% had 4 or more administrations. Not surprisingly the more immature infants were more likely to receive multiple administrations. I have to say at this point that I feel vindicated with that suggestion for late surfactant administration all those years ago as these extra doses would have been given up to days after the first dosing.
Now Here Comes The Interesting Part
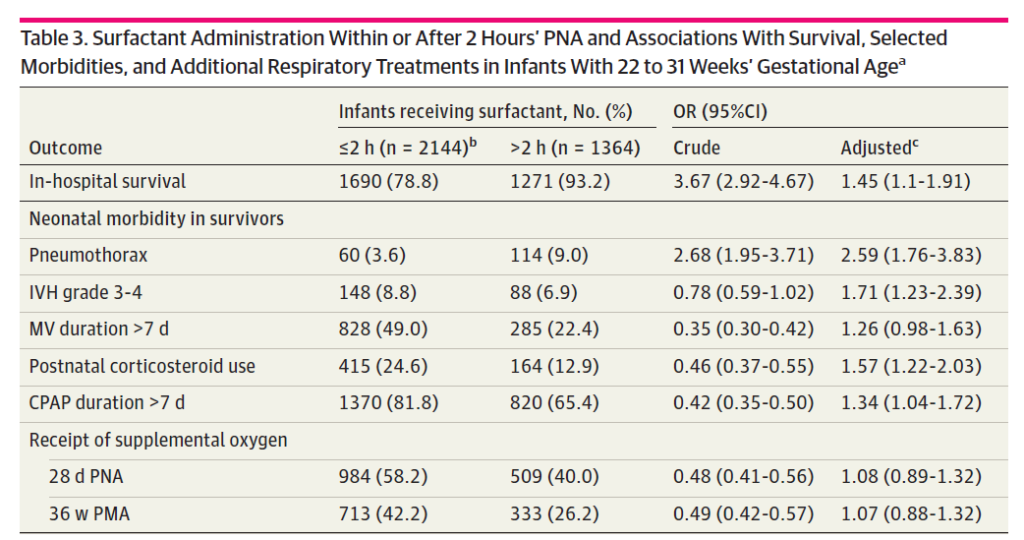
Much like previous work before this study, delivery of surfactant within the first 2 hours of age was associated with a reduction in very important outcomes of pneumothorax, IVH and need for ventilation beyond 7 days.. In short, improving compliance has a lot of benefits! The surprise was the in-hospital survival which favoured giving surfactant late. Put another way, if you receive surfactant in the first two hours you are more likely to die in hospital.
How can that possibly be if provision of surfactant has all those benefits outlined in table 3? More on that in a bit.
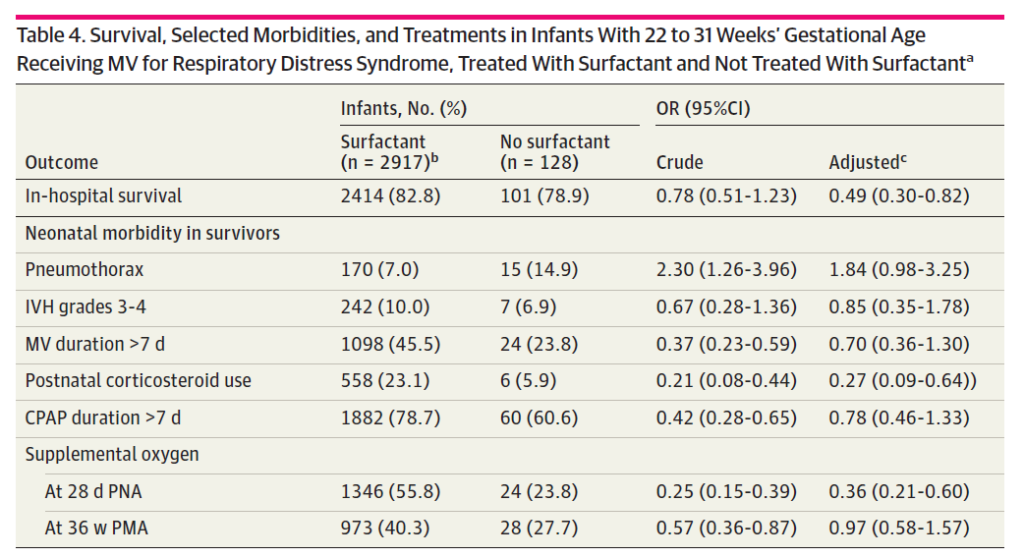
The next table addresses another question which is what if you don’t get surfactant at all? Interestinly the in-hospital survival is better for that group as well. On the other hand no difference exists for pneumothorax or IVH and ventilation beyong 7 days is improved with no surfactant at all!
The Difference Between Association and Causation
Ultimately that is what I think is at play here. You could look at the information quickly and conclude that giving surfactant late or not at all improves your chances of survival! Maybe aggressive use of surfactant isn’t such a good thing after all. I think you would be wrong there though based on prospective randomized trials. What is happening here is that the baseline characteristics are not likely equal and you are really looking at three different groups of patients.
Group 1 – These are the ones who get surfactant early within 2 hours of life. My suspicion is that the number of babies in this group that are really sick who may also have other comorbid issues is higher. There might be some babies with servere IUGR, pulmonary hypoplasia, meconium aspiration or pleural effusions that made the resuscitating team so nervous that they in advance of delivery had surfactant thawing and ready to go. Yes overall this group might benefit from better compliance and have less pneumothoraces for example but their comorbid conditions put them at higher risk of death.
Group 2 – Surfactant given after 2 hours of age. These are likely babies who are not as sick as group 1. Maybe they are babies initially managed with CPAP or NIPPV who due to escalating FiO2 requirements get surfactant. Much less likely to die.
Group 3 – No surfactant needed at all. The reason there might not be a difference in the major morbidities is that while they have RDS, TTN or MAS they are mild in nature. Clearly very low risk of death here and for that matter complications.
It might have been helpful to have some meaures of acuity documented such as SNAPPE-II (Score for Neonatal Acute Physiology with Perinatal Extension-II) used as it would help us in figuring out such differences.
Overall I think the message remains the same. Give surfactant early for those with significant lung disease. What I think it adds is an awareness that repeat dosing even if off-label is being done in Neonatology. The next question will be whether this repeat dosing makes the babies better or just us!
Giving bronchodilators to preemies on a ventilator has certainly been tried before. The major issue to contend with is getting the drug to where it is supposed to be. Anyone reading who has a child with asthma knows that you should use an aerochamber when taking a puff to help with better distribution to the lung. Giving a puff or two without it largely ends up on the back of the throat. Similarly, giving puffs through an endotracheal tuberaises questions about how much of the medication winds up on the plastic tube rather than the smooth muscle of the airways where the medication is intended to be. This has been looked at in a cochrane review as well entitled Bronchodilators for the prevention and treatment of chronic lung disease in preterm infants
Can Albuterol Save The Day?
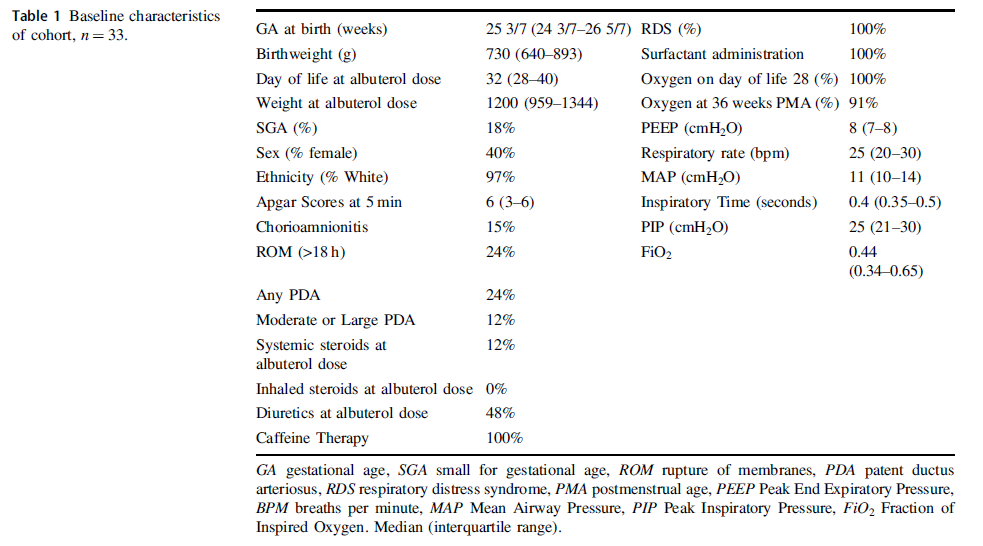
Albuterol is a beta agonist much like ventolin that can act on the smooth muscle of airways to achieve bronchodilation. Considering that preemies with immature lungs may have issues with both resistance and compliance, Raffay TM et al in their paper Response to first dose of inhaled albuterol in mechanically ventilated preterm infants chose to examine responsiveness in a group of 33 infants (all < 30 weeks at birth) to albuterol. Ideally, responsiveness would be done by pulmonary function testing but given that this was not possible in these infants they chose to examine other indicators of impact. After giving two puffs of 90 mcg of albeterol via a metered dose inhaler without an aerochamber the authors looked at changes in FiO2 as well as compliance and resistance measurements on the ventilator as a means of determining responsiveness. Ultimately, could they get drug into the distal airway in patients who were ventilated at about a month of age as shown in table 1 along with other baseline characteristics?
What makes this different than other studies I suppose is the use of the ventilator measurements and their use of histogram data on oxygen saturation to ascertain responsiveness to treatment. This was an observational study based on a secondary analysis of a previous study so we don’t have sham controls to compare to. Having said that by administering the medication and seeing what happens immediately afterwards it is possibile to get a sense of whether the drug had an effect.
So What if Any Effect Did It Have?
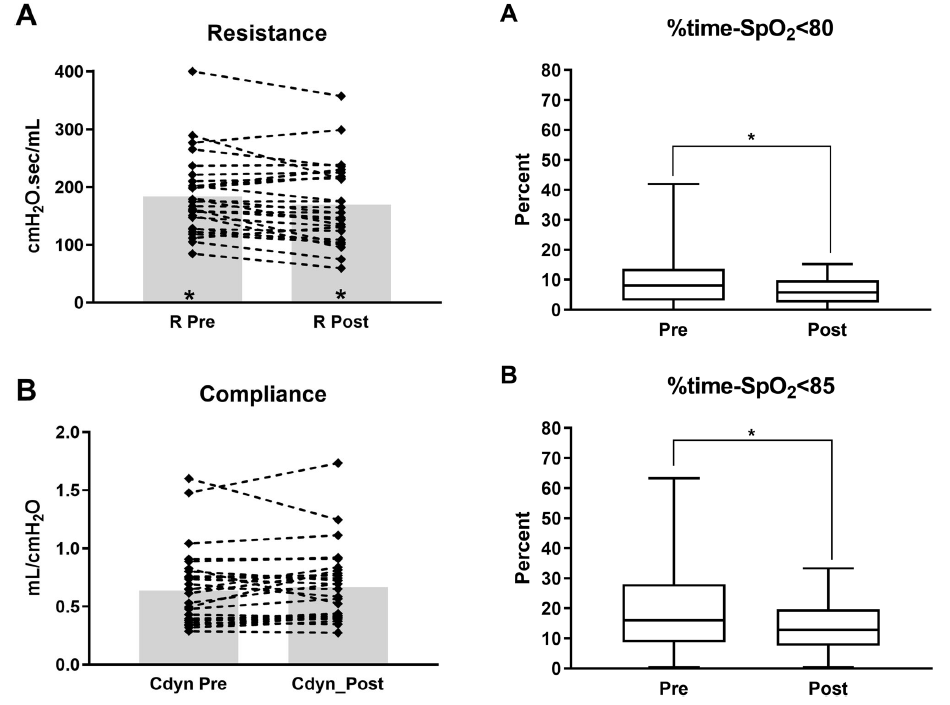
From the figure in the paper the answer is some effect. Overall, post albuterol resistance for the 33 patients overall was found to decrease. Compliance and FiO2 (not shown in the graphs below) did not change though. What did change however was the percentage of time spent below 80 and 85% respectively comparing a 4 hour window pre and a 4 hour window post with respect to histograms from the patient monitor.
Putting it together
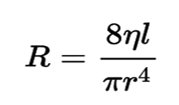
Ok so this isn’t a gold standard RCT looking at placebo treatments vs albuterol. It is hypothesis generating though as if resistance was decreased by albuterol one could expect improved delivery of O2 to the distal alveoli and therefore better oxygenation which is what is seen here. Should we be surprised that no difference in compliance is seen with albuterol therapy? I don’t think so as the effect of the drug is not on the distal alveoli and parenchyma but rather the more proximal branching airways. SInce airway resistance is governed by Poiseuille’s Law (you thought physics was over in high school?!) you can see that resistance (R) is directly proportional to the viscosity (n) and length (l) of the airway but inversely affected by the radius (r) to the 4th power. In other words if the radius of the airway after albuterol increases by 25% that effect is amplified to the 4th power in terms of reducing resistance.
I suppose I am buying what they are selling here but again the key is finding a method of getting the drug to deposit not in the trachea or proximal bronchi but to the lower airways. I can’t help but wonder if use of high frequency jet ventilation which carries flow down the centre of the airway might be a very effective way of getting such puffs further into the lung. Speculation of course but perhaps someone a little more creative than I can figure out how to do that and test deposition.
Should we use this routinely? Probably not as an everyday approach but it does make me wonder about those babies who are having a bad day so to speak. If one can glean from the ventilator that resistance has increased from one day to another might this be something worth trying? The authors found that the first treatment was effective but second and third not so much so to me this may just be a “hail mary” that is worth trying when nothing else seems to be working to reduce FiO2 in the presence of increased resistance.
If anyone is doing this routinely I would be curious in hearing your own experiences.
If you work in Neonatology you talk about caffeine endlessly whether addressing your own consumption or that of your patients. Our unit like many others typically starts caffeine early in a prophylactic fashion for babies under 32 weeks. The reason for this is due to the high incidence of apnea (AOP) in this population. The incidence of AOP follows an inverse relationship with GA, affecting 50% of those born at 30 weeks versus 7% at 34-35 weeks. Using caffeine in a more therapeutic approach is certainly sensible for babies older than 32 weeks given the lower likelihood of events. People who argue for a prophylactic strategy cite lower incidence of BPD and PDA from the CAP study while those on the side of reserving treatment for those who really need it put more emphasis on potential adverse effects such as polyuria, tachycardia and electrolyte disturbances. I have already revealed my bias as our centre takes a prophylactic approach but the question is whether it is still right given that the CAP study was many years ago now. A new study emerged this week that was shared on Twitter and generated some interesting discussion. So interesting in fact that I thought there was no better place to discuss this paper than here.
Head to Head Comparison
Elmowafi M et al published Prophylactic versus therapeutic caffeine for apnea of prematurity: a randomized controlled trial this month. This trial included 90 infants in the prophylactic arm (caffeine started < 72 hours of age) vs 91 in the therapeutic arm (only started in presence of apnea or if a baby needed mechanical ventilation and all infants were under 32 weeks of age at birth. Unfortunately, while the study was prospecitve it was not blinded although the authors state that in the therapeutic arm a neonatologist who was not part of the study team made the diagnosis of AOP. Caffeine dosing was standardized using the citrate form at 20 mg/kg as a load and with 10 mg/kg maintenance dosing (divide by 2 for base equivalents).
The primary outcome was total duration of oxygen support and a sample size was chosen based on a previous pilot RCT and the expectation that they could show a reduction in O2 requirement of 7 days in the prophylactic group. Looking at the baseline characteristics of the groups the only difference was the median day of starting caffeine which for the prophylactic group was day 1 and for therapeutic day 3.
Results
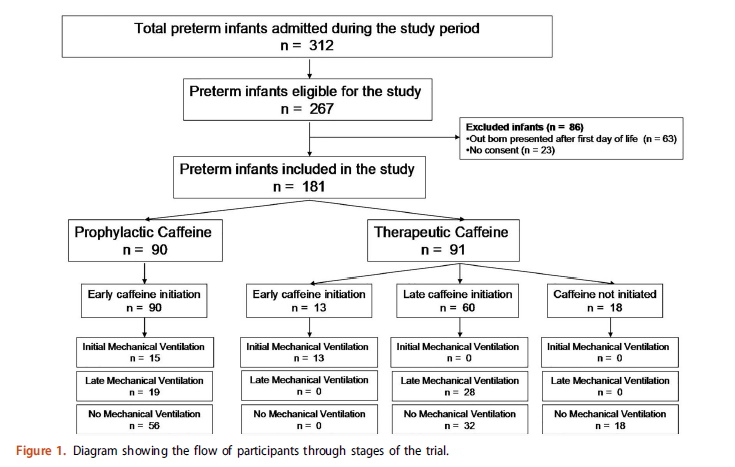
What happened in both groups and the reasons for starting caffeine are shown in teh following diagram.
As you can see, 13 patients were started due to need for initial mechanical ventilation, 28 for late mechanical ventilation with the rest being apnea as a reason except for 18 patients who never needed caffeine. When looking at the whole patient population the primary outcome was no different between the groups using an intention to treat analysis.
What the authors did next is where the controversy comes from but has some interesting data nonetheless. They did a “per-protocol analysis” on the whole group and found the following:
Per protocol analysis showed that prophylactic caffeine therapy was associated with a significant reduction in the duration of oxygen therapy compared to therapeutic initiation among included preterm infants [median and IQR of 28 (18–36) days versus 34 (23–51) days, p¼.005 respectively].
Essentially what this means is they said let’s exclude those babies who never needed caffeine and just compare babies that all received caffeine in either arm. Now they see a difference of 6 days which is pretty close to the 7 days expected . Purests will note though that by doing so you can’t claim that the groups were balanced in terms of risk factors since the presented baseline characteristics are not necessarily still the same.
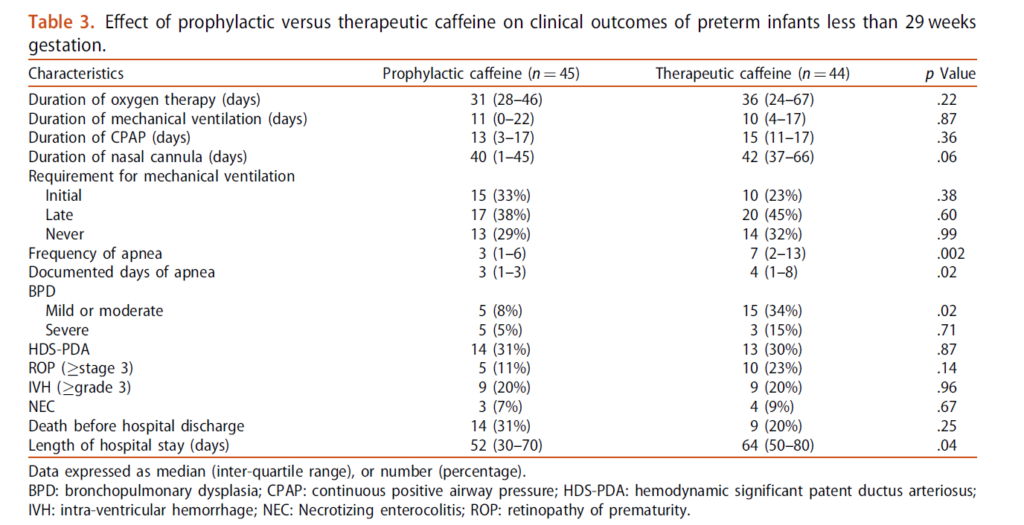
They went further though and asked the question. “What about a subgroup of <29 weeks?”. These babies are undoubedly higher risk for AOP and ventilation. Is the problem that the inclusion of babies 30-31 weeks diluted a potential benefit? Here is what they found.
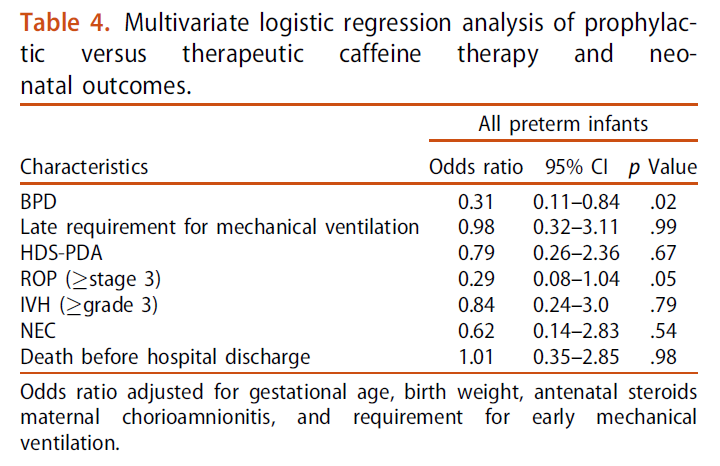
The main two things to draw your attention to are the marked reduction in mild to moderate BPD and shorter length of stay in hospital. Moreover when they looked at risk of BPD for the whole group they found a reduction in risk. Importantly there was no difference in adverse effects from caffeine use in either arm of concern.
What Can We Take From This?
Any discussion about adverse effects needs to acknowledge that these are short term outcomes we are looking at. Do babies who have never received caffeine do better in the long run? The CAP study did not suggest that was the case but it was a different time with different babies. Do I think caffeine is harmful? No I don’t, especially in the babies who would otherwise experience multiple apneic events or prolonged ventilation.
What this study does raise in my mind though is whether a change in approach to prophylactic caffeine is warranted. The authors don’t specify (I don’t think) but I suspect the bulk of the babies who did not need caffeine were in the 30-31 week group. We know that positive pressure ventilation is harmful to the developing preterm lung. Providing caffeine in the first few hours of life in the hopes of avoiding invasive ventilation or shortening the course of ventilation is the main reason that we likely see consistent reductions in BPD with its use. Under 29 weeks I would certainly favour giving caffeine early but above that as the risk of BPD drops considerably is a watch a wait approach a reasonable one to take? As this study was unblinded it is possible the babies were treated differently with respect to ventilation and apnea managment but I do think the risk is low. If the attendings caring for the babies were not part of the study and knew they were free to give caffeine if needed there may be less risk of bias.
In the end the results of this study in essence are supportive of my practice. I suspect they support many others as well. To answer the question really about side effects I suspect we would need much larger sample sizes than this with adequate power to detect differences but for now I will continue to say “give it and give it early!”
I recall the shock waves through the neonatal community when ILCOR changed its recommendation to stop routine intubation of non-vigorous infants born through meconium. The rationale again was that for most practitioners it would be better to give bag valve mask ventilation and establish a functional residual capacity than try and intubate and start with a collapsed lung.
Oommen VI et al wrote a brief report on their experience in the UK with the change as recommended for these infants. Their brief publication has a large cohort that is looked at and one result in particular I found interesting enough to share with you today. The publication is Resuscitation of non-vigorous neonates born through meconium-stained amniotic fluid: post policy change impact analysis. The authors looked prospectively at the “new approach” group from October 2016-September 2017 and compared their outcomes to the retrospecitve cohort in the same hospital from August 2015-July 2016 as the “old approach” group.
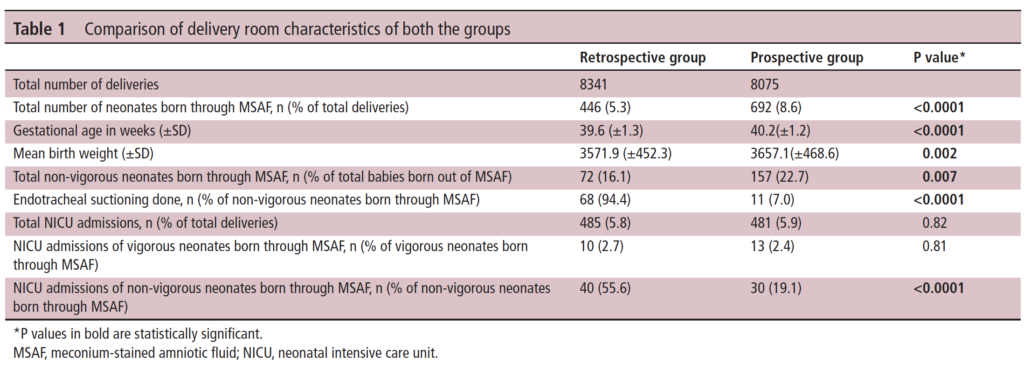
As you can see in Table 1 they saw a lot of deliveries during this time that were complicated by meconium. This gives us a good before and after comparison and while not all prospective and ensuring that practices were otherwise the same it is a pretty decent sample to look at. I like seeing that 7% of the group in the new approach still received endotracheal suctioning. It is worth remembering that what the recommendation says is to not do this routinely but if the resuscitation is not going well and the baby not responding to ventilation it is reasonable to apply suctioning as they would have done to see if there is any obstructive material in the airway.
It is the last comparison in Table 1 though that drew my attention. Over 50% of the non-vigorous babies needing routine suctioning in the retrospective arm needed NICU admission compared to 19.1% of the new approach group which was quite significant. More on this later.
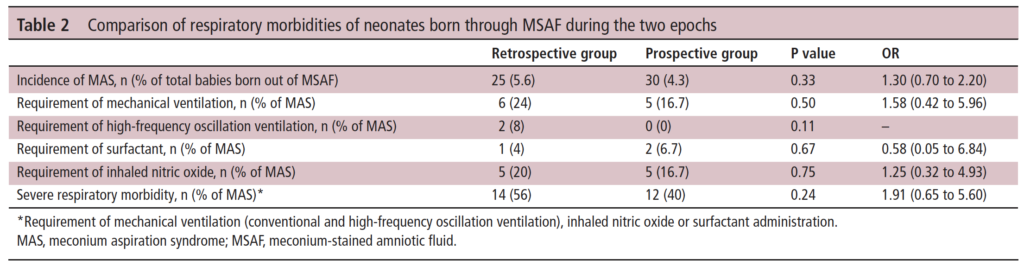
In Table 2 the authors compare the respiratory morbidities showing no difference in rates of ventilation, HFOV, surfactant or iNO. What they are demonstrating is that to the best of their abilities the babies were similar in terms of respiratory morbidiites in a binary sense. What I mean here is that when you ask the question did they need any of these aforementioned things it is a yes or no. What is not easy to pick up from the table is the quality of the respiratory disease. In the table they make it clear that severe respiratory disease was the same at 56% pre and 40% post and of course all of these babies would have needed admission. What we don’t know is what happened to the mild to moderate group.
A Theory
The whole point of giving PPV for the non-vigorous infant is to establish FRC. In the old approach it is conceivable that some of the infants could have lost volume during attempted intubation. The resultant delay in oxygenation could exacerabate any tendency to pulmonary hypertension. It could also turn a baby from one that could have had mild grunting to one that needed CPAP. Put another way it could have changed the outcome from a baby that needed observation and some prone positioning for a few hours to one that is committed to admission.
What these results show is basically what the intent of doing away with routine suctioning was supposed to do. The vast majority of severe disease in meconium aspiration syndrome is acquired in-utreo. Hypoxia and acidosis contribute to pulmonary hypertension while gasping respirations lead to inhalation of meconium deep into the airways. Suctioning after birth is not really going to help this cohort much. Providing positive pressure ventilation to the more mildly affected infants however may help open their lungs whereas delays in initiating would have the opposite effect.
In the end routine suctioning was a dogma that was in need of a challenge. The authors in the body of the paper go through other similar studies and in all but one the findings are similar. I commend the authors here for their humility as they do add at the end of the report all the potential shortcomings of the research. I for one don’t think it was necessary, as well designed research and thought went into taking down the dogma of routine suctioning. There is complete biological plausability for the findings presented here and I for one am glad to see that research in this case informed practice change that I believe was for the better.