Over the last number of years clinicians have sought more and more to limit the experience of babies to painful stimuli. In the area of surfactant administration this has focused on “less invasive” strategies such as use of small catheters while on CPAP (LISA or MIST) and surfactant via LMA or Surfactant Administration Through Laryngeal or Supraglottic Airways (SALSA) as it is sometimes known. Intubation Surfactant Extubation (INSURE) while not generally included in the less invasive approach is to a degree fitting since it involves at least intubating for a very brief period after surfactant is administered. SALSA has been growing in popularity due to its “extreme” non-invasiveness since babies are receiving surfactant without instrumentation of the airway at all. It should come as no surprise then that head to head comparisons will be done to determine which should be reigned king!
The Contenders
A group out of Albany, NY has looked at SALSA vs INSURE before in which they used morphine for premedication prior to the procedure. You might ask why any premedication is needed at all but I would suggest that covering one’s airway and dripping liquid into it might cause some irritation so why not keep them calm. The authors in their paper Randomized trial of laryngeal mask airway versus endotracheal intubation for surfactant delivery found a high rate of failure in the intubation arm which more than likely was attributable to the respiratory depressive effect of the same.
This time around in the current paper Randomized Trial of Surfactant Therapy via Laryngeal Mask Airway Versus Brief Tracheal Intubation in Neonates Born Preterm they switched to remifentanil for its brief duration of action. Babies in the SALSA arm received that drug while those in the ETT group received atropine as well. The authors included infants born from 27 weeks to 36 weeks gestation who were larger than 800g at birth. This was a non-inferiority trial with the primary outcome being Our primary outcome was failure of surfactant therapy to prevent the need for invasive mechanical ventilation or its surrogate indicators, namely, more than 2 doses of surfactant therapy, sustained need for FiO2 >0.60 to maintain target O2 saturations, or a second dose of surfactant within 8 hours of the first dose.
Surfactant redosing criteria were the same for both groups: FiO2 >0.60 or FiO2 >0.30 with clinical signs of worsening RDS. If surfactant needed to be given a second time it was via intubation. The decision to ultimately intubate though was in the hands of the practitioners.
Unfortunately, the trial was stopped after only 51 patients were enrolled into the LMA and 42 into the INSURE groups respectively. Randomization was by block design and the authors were looking for 130 patients per group so they fell far short of that. The reasons for falling short were interesting as they demonstrate one of the challenges of research and changing beliefs. At the start of the trial there was equipoise among practitioners with respect to the two modes of surfactant delivery but part way through people preferred SALSA. The authors changed the randomization to try and deal with that to a 2:1 favoring SALSA but with the combination of that and COVID they had to stop. They did manage to get enough though to determine the primary outcome in spite of this.
What did they find in the end?
Well first of all it is worth noting that there were no differences in baseline characteristics between the two groups. As it turns out, while the numbers were small it didn’t seem to lead to an unbalancing of groups.
With respect to inferiority the finding was that it was in fact not inferior as per the figure below.
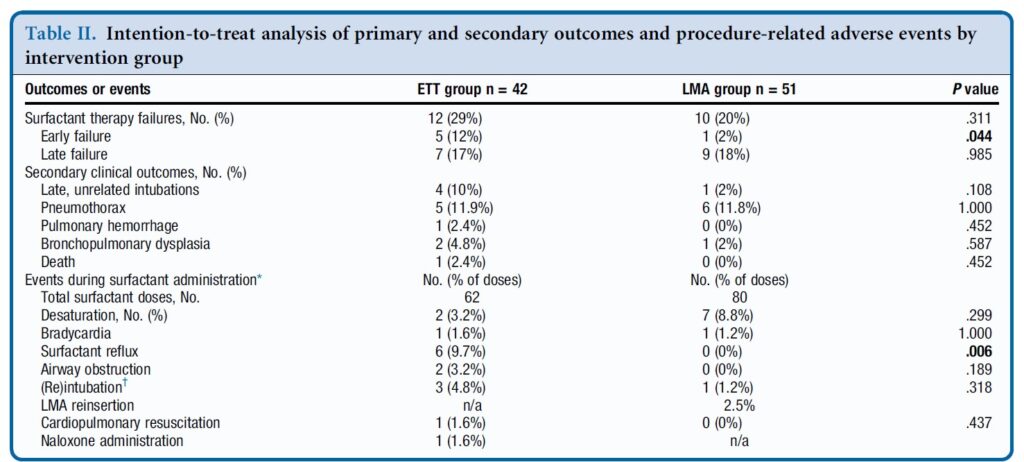
In table 2 some interesting findings emerge
Early failure of surfactant which was defined as within 1 hour of surfactant administration was found to be significantly increased in the intubation group. Late failure through at 5 days of age was not any different. An early failure is suggestive of the procedure not working to deliver the surfactant. When you look at the bottom half of table 2 the answer may be there. As part of the planned procedure the authors aspirated a gastric tube after surfactant administration to ensure that it went to the right place. There was no difference in surfactant volume aspirated via this route. There was however 9.7% of infants in the ETT group that experienced reflux in the ETT vs zero with observed reflux in the SALSA group (in the mouth perhaps?). Is surfactant without PPV better tolerated maybe?
There was a trend overall to more failures in the ETT arm although this was not found to be significant either in the intention to treat or per protocol analysis.
Where do we go from here?
First off it is important to look at who was chosen for this strategy. You may have noticed that there were no micropreemies in this trial. The reason for this is likely two-fold. The first is that prior trials on SALSA have found it doesn’t work as well to prevent intubations in babies below 27 weeks. This is very similar to the findings of studies using aerosolized surfactant. It may well be that there just isn’t enough of the total dose getting to the alveoli. If you can get some of the dose in deep into the lung for those with less severe RDS it may work ok for those babies. The second reason likely has to do with using LMAs in those in that weight range as they generally are designed for larger preemies although I understand smaller ones are becoming more readily available.
The second point is that this was not a blinded study. This could have become an issue as the authors acknowledge that there was a growing institutional preference for SALSA as the study went on. If the Neonatologist subconsciously believes it is better, might that have influenced some of the decisions to intubate again since one of the criteria was “clinical signs of worsening RDS”. It is quite possible this could have led to a few more intubations in the INSURE group for repeat doses. We can’t prove that but it is a weakness of the study.
At the very least it can be argued that the use of SALSA works as a small percentage overall failed the procedure. The largest groups of infants though were above 29 weeks so we also might not expect a high rate of failure after one dose though. It works but how well is tough to say.
Where I think this study is really important though is what it tells us for centers in particular who don’t intubate as often. Intubation is a skill that is declining in opportunity, both because of a turn to more use of non-invasive support as a primary mode of treatment. It also has become scarcer at an individual level due to there being more practitioners who can perform the skill. Having an option to use SALSA for those who aren’t as comfortable with intubation will no doubt be of much interest to many in this situation.
What is no doubt going to come next is the LISA/MIST vs SALSA trials. I hope that in the future pain scores are included in these sorts of analyses to really determine if in being less invasive we are also ensuring that we are also not undertreating discomfort. I suppose the lesson being learned from all of this is that less very well may be more.
Anyone who has watch the delivery of a baby knows that in some cases things go very smoothly and in others every care provider in the room would likely have tachycardia themselves. In some cases where labour is quite prolonged and some degree of cephalopelvic disproportion exists, the fetal head can become quite wedged in the pelvis. When this occurs it is not uncommon to hear of an ob/gyn having to dislodge the entrapped head from below and then perform a c-section to get the baby out safely.
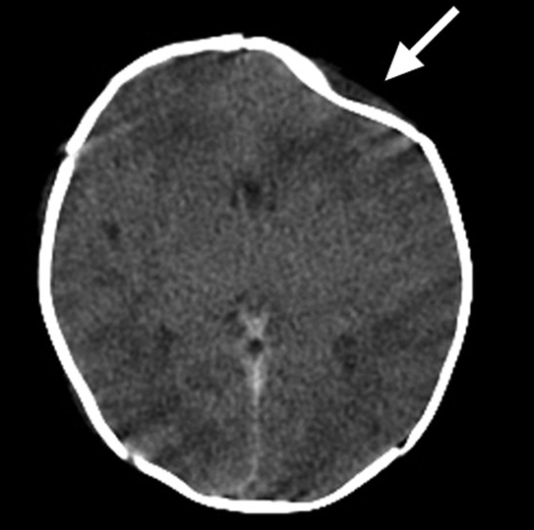
In some of these cases though on the newborn exam a depression of the skull is found such as with the figure on the right. As our brains like to link things together we may jump to the conclusion that the pressure exerted on the head from below led to a fracture. This fracture in turn may lead to injury to the underlying brain. At least that is what our brains want us to think but what if the reason for the fracture has nothing to do with the maneuver as described?
Spontaneous Skull Fractures
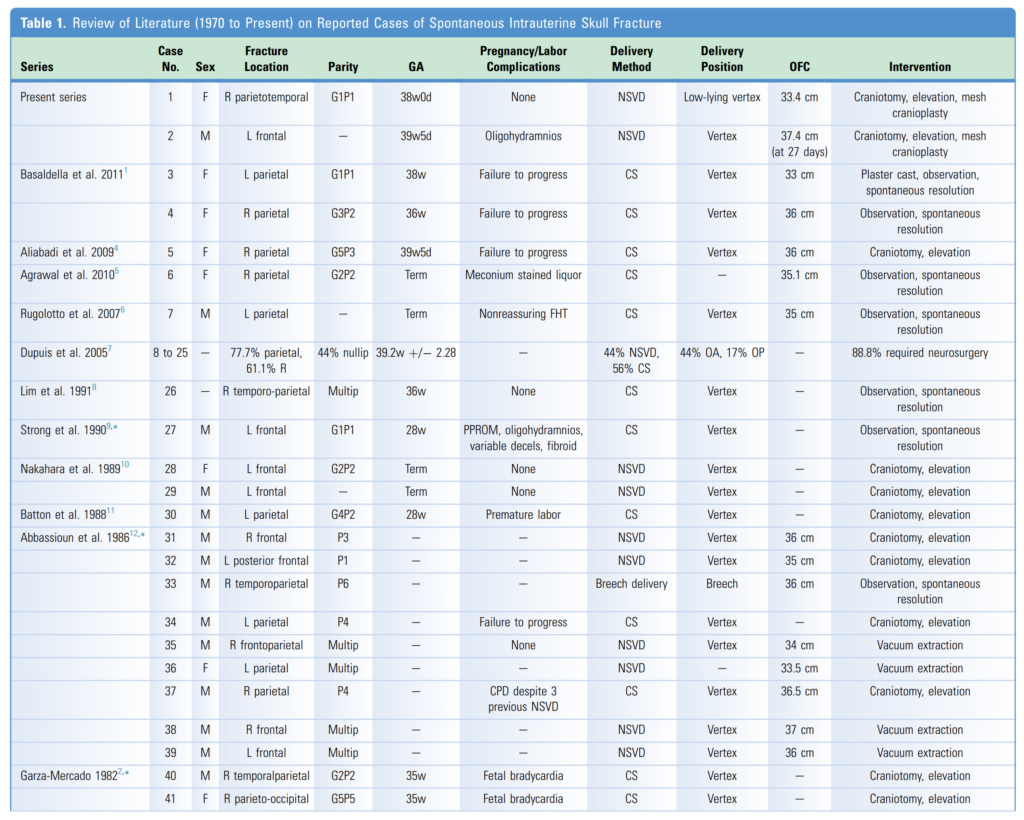
This exact situation has been described in two cases and with a review of the literature in a paper entitled Spontaneous Intrauterine Depressed Skull Fractures: Report of 2 Cases Requiring Neurosurgical Intervention and Literature Review. In this report they describe two cases, the first of which was a term infant born via SVD without instrumentation and was described as atraumatic. The figure above was from this infant and thankfully the underlying brain was free of hemorrhage. The second case was also term and again there was no need for forceps or vacuum. In this case there was significant parietal fracture with a small amount of subdural blood collection. This infant unlike the other one due to significant depression required neurosurgical intervention to correct the skull deformity and lift the bone off the brain. As the authors go on to describe there have been 39 other such patients described in the literature with the features as shown in the table from the paper. While there are 4 more in the paper they had vacuum extractions so I wouldn’t count them.
Why Does This Happen?
The short answer in most cases is a tight fit! In the 1960s this was postulated that in the right occiput posterior and and right occiput transverse positions the fetal head becomes compressed between the sacral promontory and pubic bones. Other implicating factors have been maternal fibroids leading to chronic pressure on the developing skull along with oligohydramnios that may lead to fetal compression as well.
When you look at the above table though what stands out is failure to progress as an ethology. One can imagine the contracting uterus attempting to propel the fetus forward and if impacted in the pelvis the pressure on the skull may well lead to fracture.
The other thing of note is the overwhelming involvement of the parietal bone in these cases. A presentation in another bone might lead one to think of a different etiology.
As far as treatment, many of these as you can see are simply observed but in the presence of significant bleeding neurosurgical intervention is needed. At the outset it is sensible to consult neurosurgery as one never knows which ones need intervention and which ones do not.
As you can see, the presence of a fracture and a history of forceful pushing from below MAY be related to a fracture but on the other hand these may occur simply with protracted labours themselves. In these situations while it may be tempting to blame the ob/gyn we also need to ask ourselves what the alternative they had was. Should they have let the mother continue to push with the potential risk of asphyxia or potentially even uterine rupture? At some point the delivering physician needs to get the baby out and if that is what needs to be done to extract the baby then that is what they will need to do. At the end of the day one thing is for sure that we don’t know for sure what caused the fracture and as tempting as it may be to blame the ob/gyn or GP delivering a baby it just might have been spontaneous!
This is one of the most difficult things to determine. Families being given a diagnosis of asphyxia in their baby often ask the question when did this happen? For sure this is not an exact science and in my opinion it is often difficult to answer the question with certainty. There are of course situations in which we can offer an educated guess such as if there is a witnessed acute cord compression such as with a cord presentation. In many other instances though it is more difficult to ascertain.
When meconium is passed in utero it is attributed to a hypoxic insult leading to internal anal sphincter relaxation. Depending on the length of exposure to this green amniotic fluid we also know that some babies may have a green or yellow hue to them from exposure of tissues to the pigments in meconium. What do we know about exposure of tissue to meconium? It turns out not too much but I will share with you a couple of interesting papers that help to give us a clue with a window into the past to provide a best estimate of how many hours have passed since a baby passed meconium. By knowing that we can then get a better guess as to when a hypoxic event may have happened.
Going way back in time
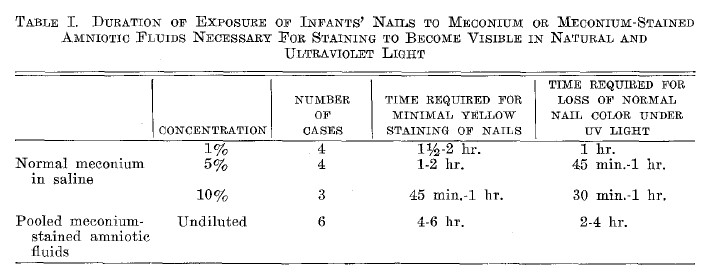
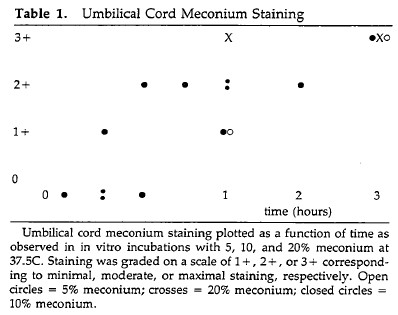
It was almost 70 years ago that Desmond MM et al published a paper trying to establish the answer to this question. The paper published in 1956 was called Meconium Staining of Newborn Infants. This paper out of Houston Texas did something that while on the surface seems disturbing was actually a creative way of determining how long exposure to meconium really takes. The authors took meconium stained fluid from 6 babies and put the fluid into sterile gloves. They then placed the feet of babies who had not been exposed to meconium into the meconium filled gloves to determine how long it took for nails to discolor and secondarily for vernix (the cheesy coating on the skin of newborns) to change color as well. The authors also created meconium slurries in normal saline of various percentages of 1 and 5% to get an idea in an artificial way with simulated meconium how long staining took. In order to determine timing of staining, at regular intervals the authors washed the baby’s feet under running water, removed the moisture with with absorbent paper, and the nails were checked for yellow staining under natural light.
As you can see from Table 1 of the paper surprisingly for natural meconium stained amniotic fluid the time it takes to stain the nails of a baby yellow ranged from 4-6 hours. This occurred faster with meconium in normal saline but for run of the mill meconium you are looking at least 4-6 hours of exposure time.
Curiously for vernix in one case it took 10 hours to turn it yellow and 12 hours in another infant.
What About Umbilical Cords and Placenta
To answer this question we need to look at another study By Miller PW et al from 1985 entitled Dating the Time Interval From Meconium Passage to Birth. in this study meconium was collected from pregnancies experiencing passage before birth and similar to the 1950s study a slurry was created in normal saline. The placenta and umbilical cord were collected from pregnancies without meconium and exposed to the slurry while being incubated at 37 degrees Celsius.
The authors in this case demonstrated that over a period of 1-3 hours the tissues subjected to the meconium slurry became stained. One might come to the conclusion that this means at least 1-3 hours is needed to stain the tissues but in all likelihood it is probably longer. We know from the previous study that an artificial slurry in normal saline seems to stain faster than meconium in amniotic fluid so it would not surprise me if the authors were to have done the study using the meconium filled glove technique the tissues might need 4-6 hours as we saw in the last study. Regardless however the point is that it takes time.
What might this mean for timing a hypoxic episode
In the absence of any meconium staining it would suggest that a baby born with meconium likely had some distress that is less than 4 hours in duration. A baby who has a stained umbilical cord, yellow nails and discolored skin has likely been exposed to meconium for greater than 4 hours. To be sure this is not an exact science but let’s say there was a labor in which 8 hours prior to delivery there were some late decelerations and practitioners were questioning could there have been a significant hypoxic injury at that time. If the infant was born with meconium staining one might argue that indeed those decelerations may have contributed to the passage of meconium. If however a baby was born through meconium and there was no staining of the tissues it might lead one to conclude that if there were a significant hypoxic event it may have occurred after that time points since there should have been staining present.
I continue to say that in these cases one cannot determine exactly when a hypoxic event occurred most of the time but the degree of meconium staining and the information provided in this piece just might help give you some added information to try and make that educated guess a little more sophisticated.
Every parent the world over waits for that moment after birth when they first hear the cry of their child. The cry is a sign of health, of vigour and a relief that all should be ok. I had never questioned when the infant cry develops but one thing is for sure, it doesn’t matter whether you are born at 25 , 30 or 37 weeks, the babies all seem to make it after delivery. Much like suck, rooting and swallowing which we know begin in utero as we can see fetal swallowing movements the question is does cry begin in utero.
Evidence for an In-Utero Start
Before I get into the answer to this let me address the title question. A cry is produced as a baby exhales and moves air in a turbulent fashion across the vocal cords. Since a fetus is not breathing air it would seem impossible for a cry to be produced by a fetus. It doesn’t mean though that a fetus can’t try to at least practice and get ready for birth.
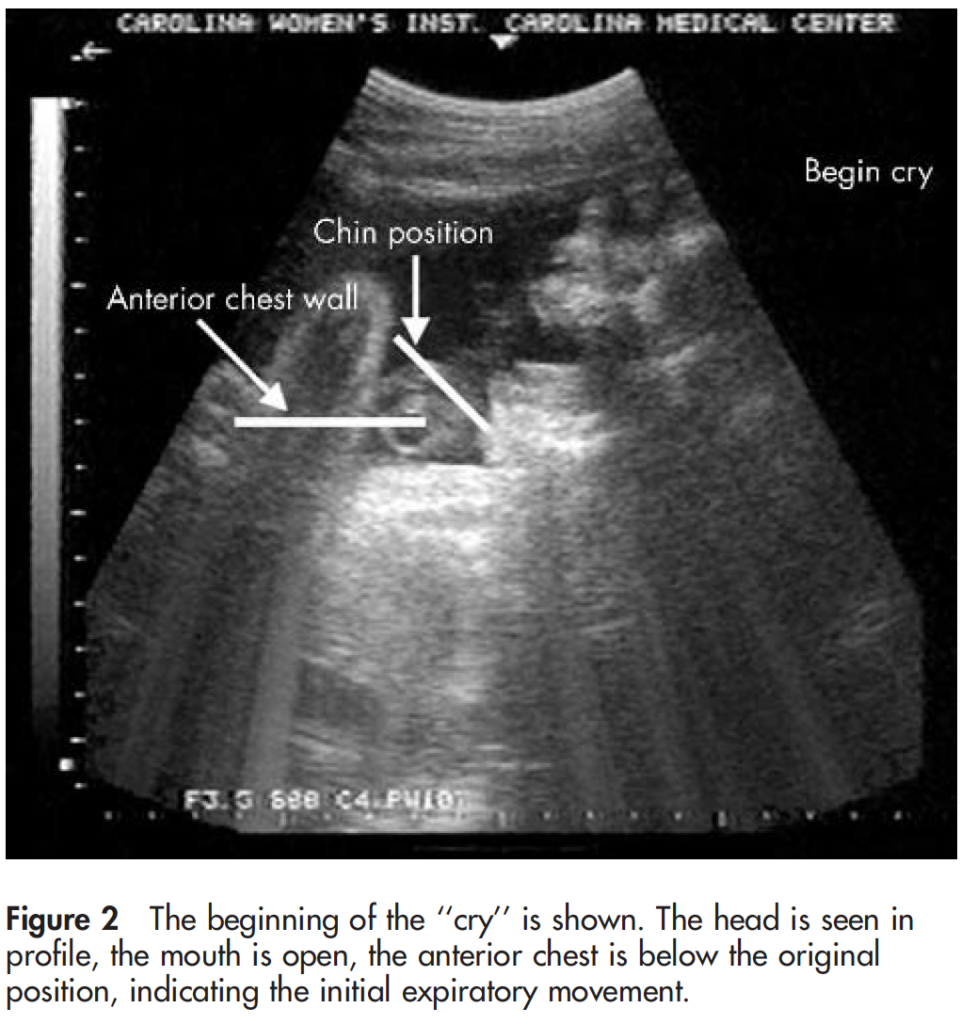
Back in 2005, a research team from New Zealand sought to answer this question in their paper Fetal homologue of infant crying. The authors described a case of a 33 week infant who was exposed to an artificial larynx generating a sound on the maternal abdomen while she was undergoing an ultrasound. The artificial larynx produced a vibroacoustic stimulation (VAS) after first keeping monitoring the fetus with ultrasound for a period of 20 minutes. The duration of the VAS was for 40 seconds and during this time the fetus was found to turn its head upon hearing the VAS and appeared to startle.
As per the authors the fetus underwent the following steps after the stimulation.
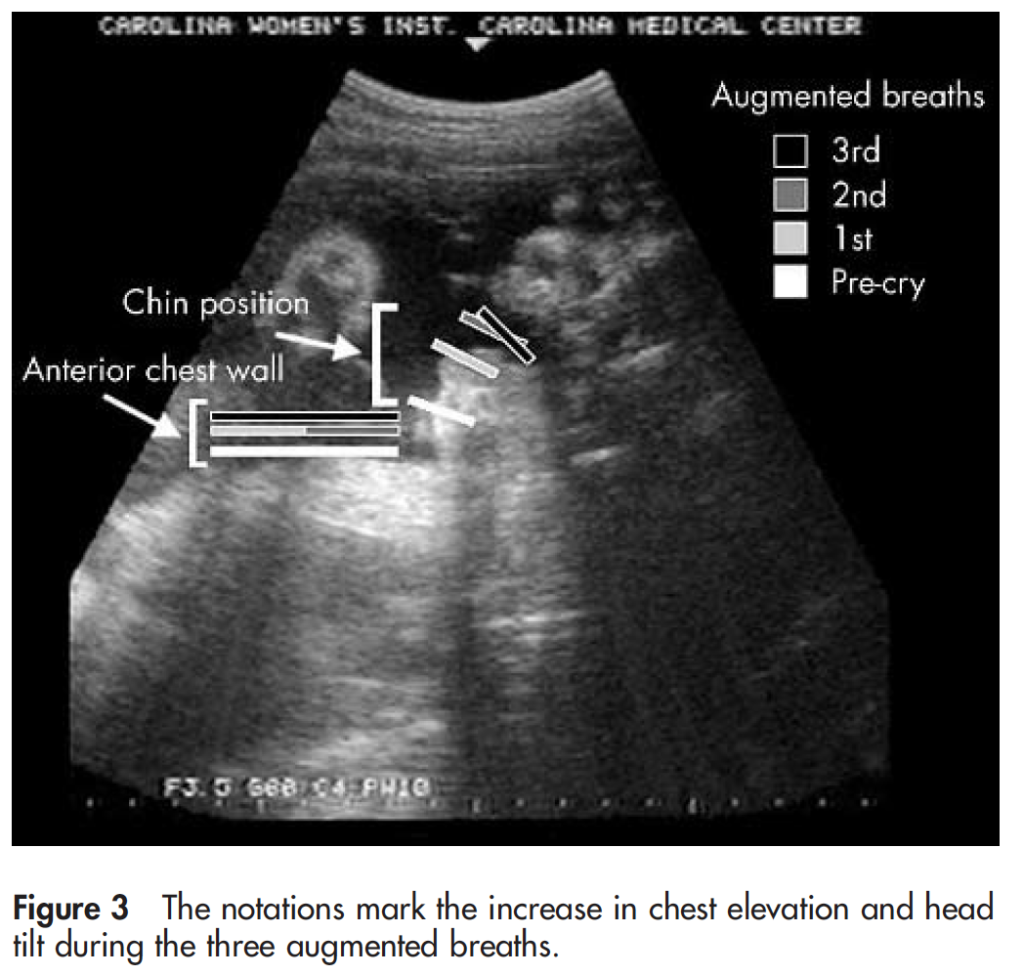
“There is a brief expiration that is followed by a deep inspiratory phase with a subsequent pronounced expiratory phase. This expiration is associated with jaw opening, taut tongue, and chest depression (fig 2). It is immediately followed by three augmented breaths with progressive increase in chest rise and head tilt (fig 3).”
At the end of this episode the chin was found to be quivering. This as I see it is the best and first description of fetal crying. While it doesn’t make a sound I believe at least that this is the beginning of an important step in development that will prepare the infant after birth to clear its lungs and inflate them with air.
The question now I ask is when does this develop? As I mentioned earlier the ability to cry is definitely present in preterm infants at pretty much any gestational age I have seen all the way down to 22 weeks. Much like other reflexes present at birth and the swallowing function mentioned earlier this must develop for a reason and I am hopeful that future work will uncover when this first appears and eventually add an explanation of what function this in-utero crying movements serve!
For commentary on this including a video of the first and second cry for this infant have a look at the full video below
I couldn’t think of a better topic for World Prematurity Day 2021 than what constitutes the edge of viability. Thinking back over my career, when I was a resident and fellow infants born at 25 and 26 weeks were deemed about as low as “we should” go but we certainly resuscitated infants at 24 weeks but this was considered heroic. Jump ahead to the last decade and we began caring for infants at birth at 23 weeks so commonly that the thought of offering comfort care only to infants at 24 weeks became almost unthinkable for many health care providers. Before I get jumped on, let me say that I am not saying I agree or disagree with that sentiment but it is something that is felt by many.
The Shared Decision Model
In the last few years a rethink again has occurred whereby the concept of the treating team knowing best has been replaced by the “shared decision model”. In this line of thinking, it is not up to us as health care providers to “tell the parents” what to do but rather come to a shared decision based on an assessment of the wishes and values of the parents in conjunction with hearing about both short and long term problems their infants may face if resuscitated. This concept was central to the statement by the Canadian Pediatric Society that I am proud to have been part of with respect to its development. The statement for those that are interested is Counselling and management for anticipated extremely preterm birth
What’s next? Going below 22 weeks?
The challenge of the shared decision model is that there comes a point where the answer is simply “no”. If for example a family at 19 weeks gestation demanded an attempt at resuscitation I would have to inform them that survival is not possible (assuming ultrasound confirmed anthropometric measurements consistent with that age). The question though becomes a little more difficult to answer at 21 weeks and was the subject of a recent article in the New York Times about a survivor at 21 weeks gestation.
Even with the best gestational age dating the estimate can be off by up to 5 days so it’s possible that the infant in this story was closer to 22 weeks or even midpoint between 22 and 23 weeks in reality. Regardless it does raise the question about what to do at 21 weeks and I suspect we will begin to see more stories about this now that the glass ceiling of 22 weeks has been breached. What about below 21 weeks? Sounds impossible I know but with research that remains at the stage of animal studies this may become possible. Maybe not in the next 5-10 years but it could happen in my lifetime in this chosen field.
The Artificial Placenta
This made headlines a few years ago with the news that the Children’s Hospital of Philadelphia had successfully kept a lamb alive for a period of 4 weeks using an artificial placenta and amniotic fluid.
You might think that this was a one-off experiment that will never see the light of day but similar work is being done in Toronto, Canada where they have been able to do similar work with preterm piglets in their paper Achieving sustained extrauterine life: Challenges of an artificial placenta in fetal pigs as a model of the preterm human fetus. Incidentally as my colleague Dr. Ayman Sheta worked on this project while in Toronto I am particularly pleased to share this research. Similar to the experience in CHOP the team in Toronto has been able to keep piglets alive for progressively longer durations. My understanding is that despite the best efforts infectious complications over arise limiting how long one can sustain such animals.
This leads me to my final thoughts on where we might be able to go. I see a future where we apply such technology to humans but not in the way that people might have thought. Keeping a fetus after delivery at 21 or 20 weeks on an artificial placenta for many weeks is not likely a realistic goal. What if we could get 1 or 2 weeks though and allow the fetus to be oxygenated without using positive pressure on their developing lungs and transition them at 23 or 24 weeks gestation? We may in this way be able to allow for postnatal maturation in a artificial uterine environment and give babies a chance who would otherwise never had the opportunity for a shared decision with medical staff.
Sound like science fiction? Well the beauty of the internet as my friend told me today is that once it’s out there it out there for good. Let’s see how this post stands the test of time and to all the babies out there in NICUs and to their families I wish you all a good and uneventful World Prematurity Day wherever you may be!