

First off I should let you know that we do not do transpyloric feeding for our infants with BPD. Having said that I am aware of some units that do. I suspect the approach is a bit polarizing. A recent survey I posted to twitter revealed the following findings:
I think the data from this small poll reveal that while there is a bias towards NG feeds, there is no universal approach (as with many things in NICU).

Conceptually, units that are using transpyloric feeds would do so based on a belief that bypassing the stomach would lead to less reflux and risk of aspiration. The question though is whether this really works or not.
New N of 1 Trial
I don’t think I have talked about N of 1 trials before on this site. The trials in essence allow one patient to serve as a study unto themselves by randomizing treatments over time for the single patient. By exposing the patient to alternating treatments such as nasogastric or nasoduodenal feedings one can look at an outcome and get a sense of causality if a negative or positive outcome occurs during one of the periods consistently. That is what was done in the study Individualising care in severe bronchopulmonary dysplasia: a series of N-of-1 trials comparing transpyloric and gastric feeding by Jensen E et al from the Children’s Hospital of Philadelphia. The authors in this study determined that using a primary outcome of frequency of daily intermittent hypoxaemic events (SpO2 ≤80% lasting 10–180 s) they would need 15 patients undergoing N of 1 trials between nasogastric and nasoduodenal feeding. Included infants were born at <32 weeks and were getting positive airway pressure and full enteral nutrition at 36 0/7 to 55 6/7 weeks PMA. Infants who were felt to be demonstrating signs of reflux or frank regurgitation were enrolled.
The findings
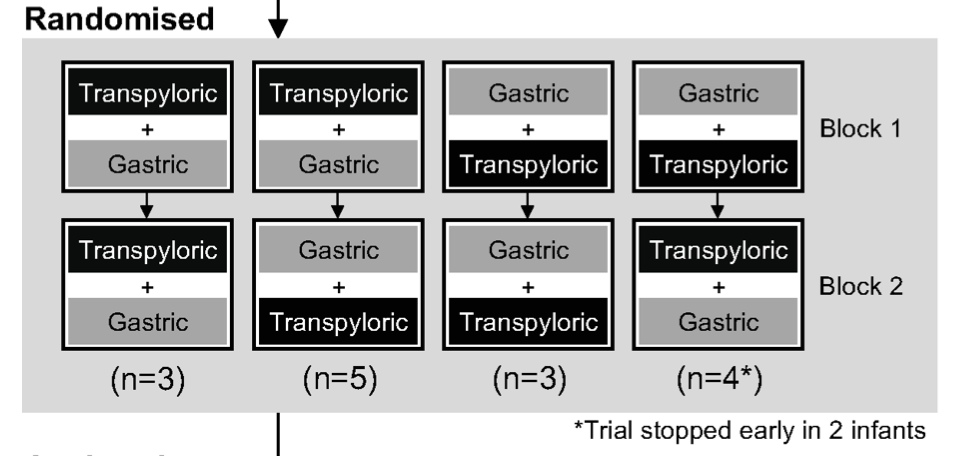
Thirteen of 15 enrolled patients completed the study. The two who did not complete did so as their oxygen requirements increased shortly after starting the trial and the clinical team removed them and chose their preferred route of feeding. Randomization looked like this:
Of the 13 though that completed and using an intention to treat analysis of the other two the findings were somewhat surprising. Contrary to what one might have thought that transpyloric would be a lung protective strategy, the findings were opposite.
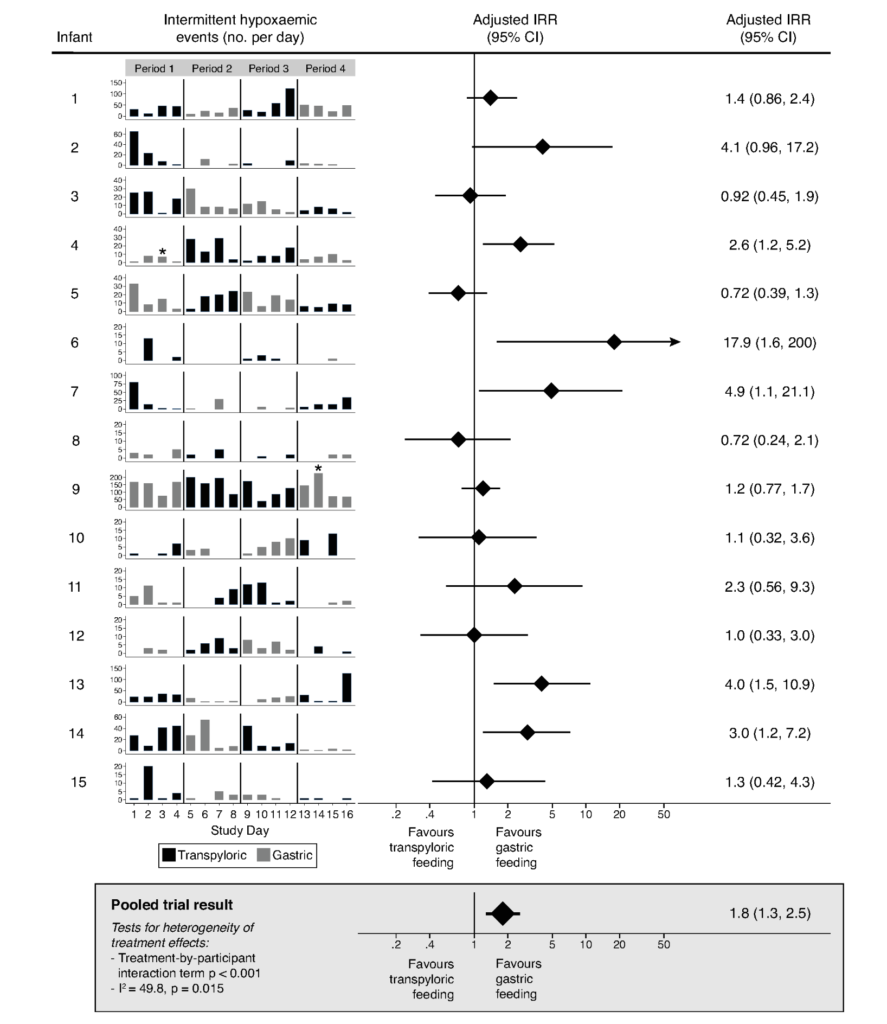
Overall the combined results from these 15 patients demonstrated that nasogastric feedings were protective from having intermittent hypoxic events.
How can this be explained?
To be honest I don’t really know but it is always fun to speculate. I can’t help but wonder if the lack of milk in the stomach led to an inability to neutralize the stomach pH. Perhaps distension has nothing to do with reflux and those with BPD who have respiratory distress with some degree of hyperinflation simply are prone to refluxing acid contents due to a change in the relationship of the diaphragmatic cura? It could simply be that while the volume in the stomach is less, what is being refluxed is of a higher acidity and leads to more bronchospasm and hypoxemic events.
What seems to be clear even with this small study is that there really is no evidence from this prospective trial that transpyloric feeding is better than nasogastric. Given the size of the study it is always worth having some degree of caution before embracing wholeheartedly these findings. No doubt someone will argue that a larger study is needed to confirm these findings. In the meantime for those who are routinely using the transpyloric route I believe what this study does at the very least is give reason to pause and consider what evidence you have to really support the practice of using that route.