

Original Post
I don’t know if you missed it but I did until tonight. We don’t have this in Canada but there have been some US states that have been doing so for the past while. You may find the following link very interesting that explains the positions of each state in regards to drug use in pregnancy. The intentions were good to protect the unborn child but the consequences to mother’s who tested positive were of great concern. While testing of mothers for drug use has been done off and on for years what made this different was that the confirmation of drug use was deemed to be a criminal offense with the results handed over to the police.
As this article from March 4th indicates the practice has been ongoing in Tennessee for at least a year and a pilot project was planned for Indiana this year. According to the article the situation in Tennessee came with some significant risk to the mother if found to have a positive screen.
“Lawmakers in Tennessee last year increased drug screenings of expectant mothers and passed a law allowing prosecutors to charge a woman with aggravated assault against her unborn baby if she was caught using illicit drugs. The penalty is up to 15 years in prison.”
The law may seem harsh and in my eyes is but it came in response to the tidal wave of drug addiction and neonatal withdrawal in the US as was identified in the article from the NEJM in 2015 entitled Increasing Incidence of the Neonatal Abstinence Syndrome in U.S. Neonatal ICUs. The impact on neonatal ICUs in the US can be seen in the following graphs which demonstrate not only the phenomenal rise in the incidence of the problem but in the second graph the gradually prolonging length of stay that these patients face. 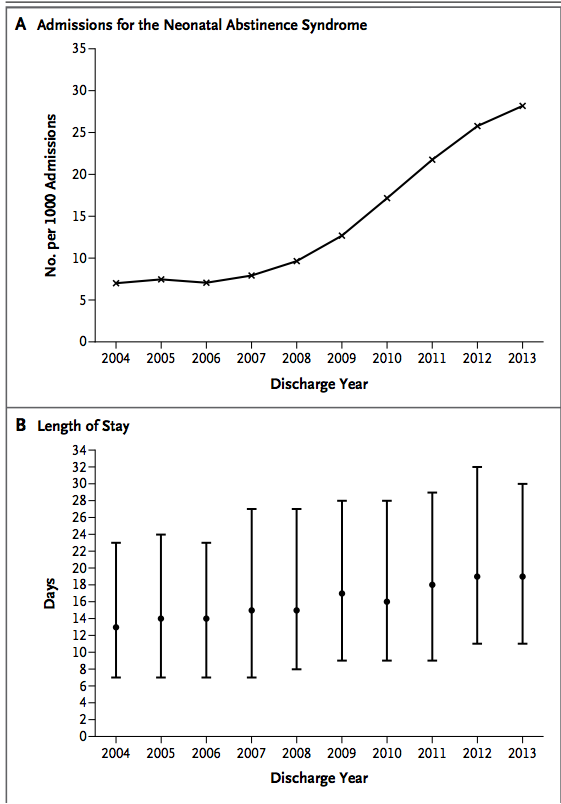 Aside from the societal issues these families face and the problems their infants experience, the swelling volume of patients NICUs have to contend with are quite simply overwhelming resources with time. Although I reside in Canada, it is the trend shown that likely motivated some states to adopt such a draconian approach to these mother-infant dyads.
Aside from the societal issues these families face and the problems their infants experience, the swelling volume of patients NICUs have to contend with are quite simply overwhelming resources with time. Although I reside in Canada, it is the trend shown that likely motivated some states to adopt such a draconian approach to these mother-infant dyads.
There are so many questions that would arise from such an approach.
- What if a mother refuses testing as is the option in Indiana. Would Child and Family services be called simply on the suspicion?
- What if a mother received prescription opioids for chronic back pain or used an old prescription in the days before she was tested after a fall to ease her pain?
- Then there is the Sharapova situation
 where a mother could conceivably take a medication that she is unaware is on a list of “banned substances”. What about Naturopathic or herbal supplements that might test positive?
where a mother could conceivably take a medication that she is unaware is on a list of “banned substances”. What about Naturopathic or herbal supplements that might test positive? - Then what about false positive tests?
The ramifications of any of the above situations on the family unit could be devastating. Interestingly this year the courts in Indiana passed a law that prevents health care providers from releasing the results of such toxicology screens to police without a court order so indeed there would need to be suspicion. In the end though is it right?
Tennessee Sings a New Tune
As surprised as I was to hear about the situation in Tennessee just now I was equally surprised to come across a U.S. Supreme Court ruling handed down March 21st, 2001 that has ruled that subjecting mothers to such testing in hospitals is unconstitutional. This may disclose my ignorance of US law but I would have thought if the US Supreme Court says you cannot do something the states would follow along but at least in Tennessee that was not the case…until now.
March 23rd the law in Tennessee is changing as the state has chosen not to renew the legislation after a two year trial period saw about 100 women arrested. For more information on this decision see Assault Charges for Pregnant Drug Users Set to Stop in Tennessee.
Where do we possibly go from here?
I found this whole storyline shocking but I am taking some solace in knowing that this was a very limited experiment in one state. Neonatal abstinence is a problem and a big one at that. Criminalizing mothers though is not an effective solution and to me the solution to this problem will need to involve a preventative approach rather than one of punishment. A first step in the right direction will be to stem the tide of liberal use of prescription opioids in pregnancy as was suggested in the BMJ news release in January of this year. In the end if we as medical practitioners are freely prescribing such medications to the mothers we care for perhaps we should look in the mirror when pointing fingers to determine fault. So many of the mothers and the infants we care for may well be victims of a medical establishment that has not done enough to prevent the problem.
Update
While screening women presenting to the hospital in labour or their newborns for that matter may seem like a wise choice, the request to procure a sample remains just that. It is a request and in collecting consent is needed. This was the advice at least I was given by the Canadian Medical Protective Association. It does create an interesting situation though in the mother who refuses to have her or her baby submit a urine specimen. Should we assume that a woman who refuses testing is in fact using an illicit substance or is she merely choosing to not have a wasted test when she knows that she is not using anything? How do we as practitioners view this decision and do we jump to a verdict of guilt immediately? I suspect the answer is that most of us would assume so especially if we are using a targeted screening approach in which we are only approaching those mothers who we suspect are using.
The secondary question becomes the “so what”? What I mean by this is how will our management change if we know or don’t know? If we suspect use and the baby is demonstrating signs of withdrawal abstinence scoring will start. If the source of the symptoms are unknown would we not just treat with phenobarbital to cover the possibility that there is more than one drug at play here? I used to be on the side of the argument that felt we had to know and therefore pushed for such screening but in the end will it really change our management? Not really.
This past month the American College of Obstetricians and Gynecologists (ACOG) issued a committee opinion on opioid use in pregnancy. The important points to share with you are the following and I would agree with each.
- Screening for substance use should be part of comprehensive obstetric care and should be done at the first prenatal visit in partnership with the pregnant woman. Screening based only on factors, such as poor adherence to prenatal care or prior adverse pregnancy outcome, can lead to missed cases, and may add to stereotyping and stigma. Therefore, it is essential that screening be universal
- Urine drug testing has also been used to detect or confirm suspected substance use, but should be performed only with the patient’s consent and in compliance with state laws.
- Breastfeeding should be encouraged in women who are stable on their opioid agonists, who are not using illicit drugs, and who have no other contraindications, such as human immunodeficiency virus (HIV) infection. Women should be counseled about the need to suspend breastfeeding in the event of a relapse.
The issue of consent seems to be firmly in place based on this position and as I mention above I think that is a good thing. The question of breastfeeding comes up frequently and it is good to see ACOG take a clear view on this as I have often thought that the benefits of the same plus the administration of small quantities of the drug in the milk may have a double benefit in reducing symptoms.
.
My niece lives in Tennessee. She uses Meth and is pregnant with her second child. She lost custody of her first child due to Meth use and hasn’t cared to do what is necessary to regain custody. Her baby is due in September. She is 22. She refuses to get a GED, to work, and left the rehab she was in. She even refuses to get her driver’s license. So what do we do with people like this? Rehab cannot be “forced” in our country, so people continue to use. At this point, I care more about the baby & her other child that she abandoned and left with her Mom to raise (who also has drug issues). The system allowed my sister to have custody of her baby and she has all of her adult kids living with her. They all use and there have been 4 assault charges by her kids in one year and child protective services often does not even investigate. About a decade ago, a 3 year old my sister watched and cared for was beaten to death by her father’s girlfriend who was watching her at the time. The baby, Emily, accidentally knocked her drug fix off the table and the girlfriend, Amber, flew into a rage, beating the child to death. Both of Emily’s parents (despite the death of their child) continued using Meth and her father is now in prison for dealing. No one up there wants to change. They live in squalor and at one point my sister was letting the dogs crap in the floor and she had rats in her home. Her kids slept on mattresses on the floor with no sheets. She has holes in the walls of her manufactured home. Nothing you say or do in any way makes a difference.
It’s all good when you haven’t been intimately affected by addiction, but we don’t have the access to treatment here in the US and we cannot force treatment either. So, my niece is getting ready to have her second child. She has never worked. No one in my sister’s family works. Two are disabled due to the Meth use. So, what should we do then? People need to experience consequences if they choose to use and endanger the life inside of them. I’m even pro-choice and liberal (Vote Democrat), but I’m really tired of watching my entire family sit up there with crime, drugs, and assault around a child. Maybe jail will wake my niece up. She feels entitled to sit and do nothing. She dropped out of high school, refuses to work, and won’t do the things necessary to get well or to regain custody of her first child. She is a danger, in my opinion, to the child’s life.